


Docsity.com


Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Community
Ask the community for help and clear up your study doubts
Discover the best universities in your country according to Docsity users
Free resources
Download our free guides on studying techniques, anxiety management strategies, and thesis advice from Docsity tutors
Vascular Dementia, Vascular Cognitive Impairment, Spectrum of Cognitive Disorders, Executive Dysfunction, Post Stroke Dementia, Large Artery Infarctions, Lacunes, Chronic Subcortical Ischemia are some points from lecture of Introduction to Geriatrics course.
Typology: Slides
1 / 11

This page cannot be seen from the preview
Don't miss anything!
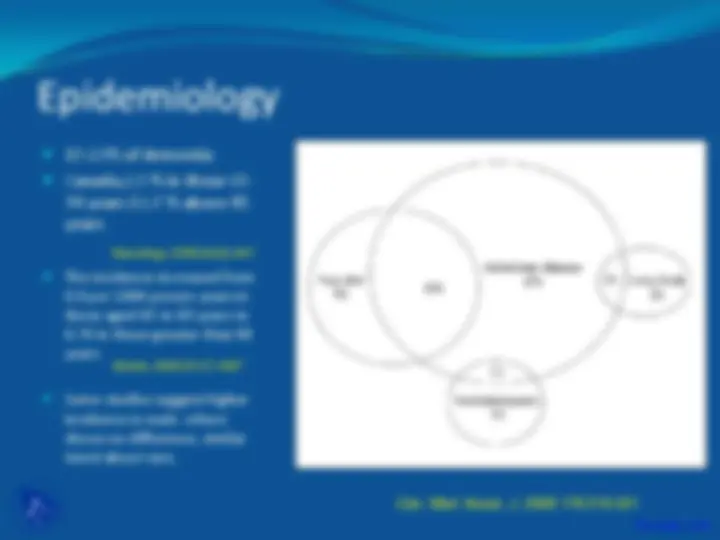
which often includes executive dysfunction. The most severe form of VCI s VaD and the Milder form is VaMCI
Stroke 2011, 42:2672-
Multiple studies shows incidence between 6-32%
Mild cognitive impairment before stroke increases the likelihood of post-stroke dementia
Age increase the risk of dementia after stroke
Timing of assessment after stroke.
Other factors, Severity of stroke, AF, WMLs, Multiple events, HTN, obesity,
Anatomic distribution: Strategic sites
Cortical (hippocampus, angular gyrus,,frontal lobe) and subcortical (thalamus, fornix, basal ganglia)
WML and the presence of dementia
Anatomic distribution
periventricular rather than subcortical WML
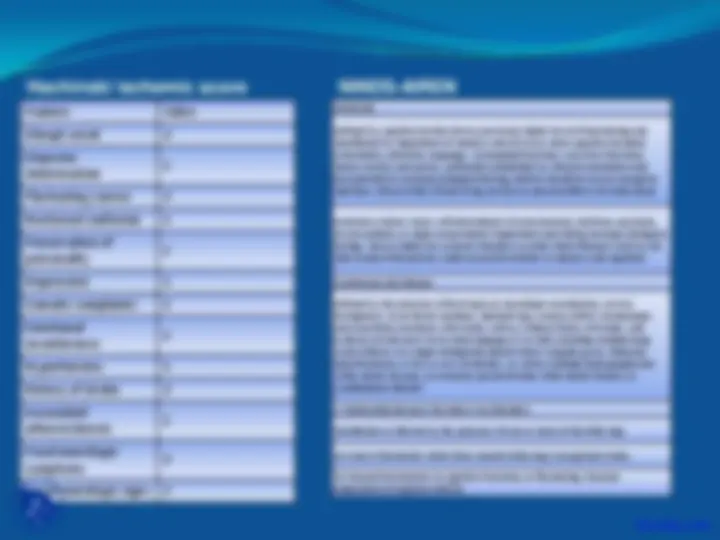
Feature Value
Abrupt onset 2
Stepwise deterioration
Fluctuating course 2
Nocturnal confusion 1
Preservation of personality
Depression 1
Somatic complaints 1
Emotional incontinence
Hypertension 1
History of stroke 2
Associated atherosclerosis
Focal neurologic symptoms
Focal neurologic signs 2
Hachinski ischemic score Dementia Defined by cognitive decline from a previously higher level of functioning and manifested by impairment of memory and of two or more cognitive domains (orientation, attention, language, visuospatial functions, executive functions, motor control, and praxis), preferably established by clinical examination and documented by neuropsychological testing; deficits should be severe enough to interfere with activities of daily living not due to physical effects of stroke alone.
Exclusion criteria: Cases with disturbance of consciousness, delirium, psychosis, severe aphasia, or major sensorimotor impairment precluding neuropsychological testing. Also excluded are systemic disorders or other brain diseases (such as AD) that in and of themselves could account for deficits in memory and cognition.
Cerebrovascular disease Defined by the presence of focal signs on neurologic examination, such as hemiparesis, lower facial weakness, Babinski sign, sensory deficit, hemianopia, and dysarthria consistent with stroke (with or without history of stroke), and evidence of relevant CVD by brain imaging (CT or MRI) including multiple large vessel infarcts or a single strategically placed infarct (angular gyrus, thalamus, basal forebrain, or PCA or ACA territories), as well as multiple basal ganglia and white matter lacunes, or extensive periventricular white matter lesions, or combinations thereof. A relationship between the above two disorders Manifested or inferred by the presence of one or more of the following:
(a) onset of dementia within three months following a recognized stroke; (b) abrupt deterioration in cognitive functions; or fluctuating, stepwise progression of cognitive deficits.
NINDS-AIREN
Treatment
Risk factor management.
Antihypertensive
incident dementia of 0.87 (95% CI: 0.76-1.00). Lancet Neurol. 2008;7(8):.
Diabetes , limited literature, higher BS and A1c- increased cog decline.
Statins. Interest b/o CV risk and pleiotropic effect on vasculature, RCT of lipid lowering does not show effect on cog. Antiplatelet agents_. No study to show benefit in dementia_
Homocysteine lowering- CV risk factor, again on efffect on dementia
Healthy lifestyle –smoking cessation , alcohol use, physical activity, and diet are associated with improved cognitive function.
Acetylcholinesterase inhibitors- beneficial in cognition, functional improvement and clinical assessment.
N-Methyl-D-aspartate receptor antagonists -memantine
Calcium channel blockers