




















































































Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Community
Ask the community for help and clear up your study doubts
Discover the best universities in your country according to Docsity users
Free resources
Download our free guides on studying techniques, anxiety management strategies, and thesis advice from Docsity tutors
This is the Tolal Salary Cost for Staff at the Facility. Each entry should be completed with a total salary for all the positions associated wilh this ...
Typology: Exercises
1 / 142

This page cannot be seen from the preview
Don't miss anything!
and Counselor lntern.
Address:
Total Hours/Week: Res¡dential % and
Enter the Facility name. Enter the Facility's physical street address, including City, State, and Zip Code. Each Facil¡ty locat¡on requ¡res a separate Exh¡b¡t J.1 to be completed.
titles on lhe job descriplions submitted. Enter all special qualifications required for êach position (these should match the job description qualifications). ln addition, for Upper Level Management (ULM) posilions, include ULM as a qualification. For each position, enler the number of hours per week spent on the Contracl at this Facility. Enter the percentage^ of time spent on the Conlract at this location, broken down by Program. Relapse %:
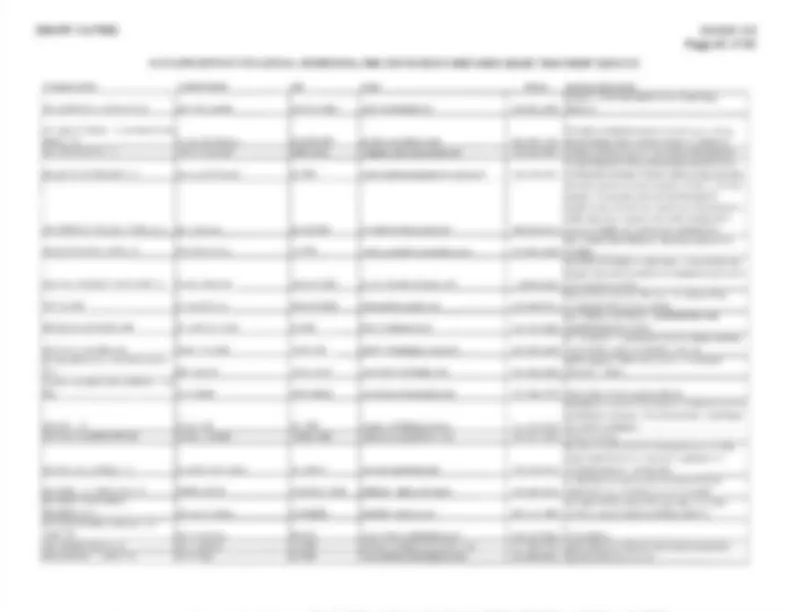
Exhibit J. STAFFING PLAN AND BUDGET JUSTIFICATION FORM REHABILITATION TREATMENT SERVICES - Phase lAdult Support¡ve Residential, TC^ lntensive Residential^ Relapse,
Fac¡l¡ty Name Address city' state' zip code (^) Note: Additionat rows are hidden and may be as needed to list additional informat¡on Pos¡t¡on Tille
Executive D¡rector
Special Qualif ications
Bachelor Degree, 3 Yrs. Exp., ULM
Tolal Hours/Week
40 00
Total FTE
Residenlial %
50%
Relapse %
50% Business Manager 2 Yrs. college, 3 Yrs. Exp., ULM 40.00 1.00 50% 50% Reception¡st HS/GED, 2 Yrs. Exp. 40.00 1.00 50% 50%
Program Director LCDC, 10Yrs. Exp., UL[4 40.00 1.00 750k 25% lntake Coordinator HS/GED, 3 Yrs. Exp. 40.00 1.00 750,$ 25% Maintenance Tech HS/GED, 12 Months Exp. 40.00 1.00 75% 250Â Counselor LCDC 120.OO 3.00 1000/6 Oo/o Counselor LCDC 40.00 1.00 o% 1000Â Counselor lntern LCDC-Ct 120.00 3.00 1 00% 00, Counselor lntern LCDC-Ct 40.00 't.00^ 0% 100% Resident¡al Mon¡tor HS/GED, 6 l\¡onths Exp. 160 00 4.00 '1000Á^ 00Á Residential Monibr HS/GED, 6 l\¡onths Exp. 80.00 2.OO 00À '1000, cook HS/GED, FH Certificate, 1 Yr. Exp. 80.00 1.00 75% 25%
GRAND TOTAL 880.00 21.
TDCJ-PFCMOD
Page I (^) of 10 Revised 8/
696-PF-19-P
Address:
COST CATEGORY / ITEM
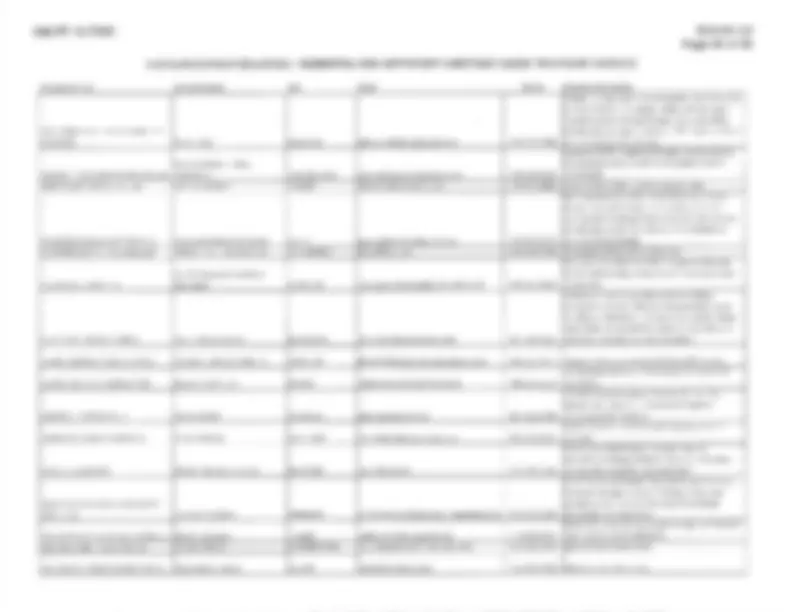
BUDGET JUSTIFICATION FORM INSTRUCTIONS To be Completed for Phase I Adult Supportive Residential Facility
Enter the Facility name. Enter the Facilily's physical street address, including C¡ty, State, and Zip Code.
percenlage (^) of time spent at the location identified on the Budget Justification. A Budget Justilication should be completed for each location.
Plan. ln these^ columns, the estimated expenditures for each individual budget line item must be entered for lhe lerm of the Contract. These are expend¡tures (^) associaled with the direct operation of the Facility, excluding salaries. These are expendilures associated with overseeing the Contract, but not directly related to lhe Facility. Enter the number of beds associaled with lhis localion.
Exhlbll J.
Galculated cells are locked and include the following: Subtotals, Grand Totals, and Operating Per Diems.
REHABIL|TAI,ON TREATMENT SERVICES - Phase, Adult Suppott¡ve Res¡dential Fac¡lity BUDGÉ1J US'IIFICATION Fac¡lity NameAddress C¡ty, State, Zip Code
CATEGORY / ITEM
D¡rector
FlEs
o.7 s
$ 60.
Yøar 2 -^ FY $ 6'i.
$ 62.
Yøar 2 - ÊY $ 63,672^ I$ 64,946 $ ø6,245^ $ 67,570^ 68,92'l ntake Coødinator o.75 (^) $ 1 5,000 $ 15,300 I '15,606^ $ '15,918^ $ 16,236 $ '16,561 (^) $ 16,892 $ 17, \¡aintenance Tech o.7s (^) $ 30,000 $ 30,600 (^) $ 31,212$ 3't,836 (^) $ 32,473 $ 33,122 $ 33,785 $ 34, lounselor 3.00 $ 90,000 $ 91.800 $ 93.636 $ 95,509 $ 97,415 $ 90,367 (^) $ '101,355 $ 103, :dnselor lntern 3.00 (^) $ 60,000 $ 61,200 s 62,424 (^) $ 63,672 (^) $ 64,946 $ 66,24s (^) s 67.570 $ 68. lesidential Mon¡tor 4.00 $ 80.000 $ 81.600 43.232 (^) $ 84,897 $ 86,595 $ 88.326 $ 90,093 $ 91, 000
190
$
$
$
$
$
$ 38,
s 37.1 63
$ 38,
$ 37,
$ 39,
o.
C6ts
$ 35
nsurance Prem¡ums (^) $ 5.000 (^) $ 5.100 $ 5.202 (^) $ 5.306 (^) $ 5,412$ 5,520 (^) $ 5,ô31 $ 5, Vlaintenance (^) $ 6,000 $ 6,120 $ 6,242 $ 6,367 $ 6,495 $ 6,624 (^) $ 6,757 (^) $ 6, Jtilities (^) s 24,000 (^) $ 24,480 (^) $ 24,970 (^) $ 25,469 (^) $ 25,578 $ 26.498 (^) $ 27.028 $ 27. )ffce Supplies $ 2,000 $ 2,O40 $ 2,O81 $ 2,122 $ 2,165$ 2.208 (^) $ 2.252 (^) $ 2, lomputer Suppl¡es (^) $ 4,000 (^) $ 4,080 (^) $ 4,162 $ 4,245 $ 4,330 $ 4,416 $ 4,505 $ 4, rostage (^) $ 150 $ '153 $ 156 $ 15S (^) $ 162 $ 166 $ 169 $ 172 -^urriculum $ 750 $ 745 $ 780 I 796 $ 812 s (^828) $ 845 $ 862 lopiers / Fax Machines $ 1,000 $ 1,020 $ 1,040 $ '1,061^ $ 1 ,082 $ 1,104 $ 1,126 $ 1 149 lelecmmun¡cat¡ons (^) $ 150 $ 153 $ 156 $ 159 $ 162 $ '166 $ 189 $ 172 =quipment $^ 2,100^400 $^408 $^ 4't6 $^424 $^433 $^442 $^450 $^450
$ 99,
$ 142
$ 100,
185
I 03,
$
$ 't05,060^ 107,
$ 2,
$
2,31S
109
$
$ 111
2,
$
$ 2,
Salãries $ 11 720 ndirect Fringe Bên€fìls (^) $ 6,750 s 6,885 $ 7,O23 $ 7.163$ 7,306 $ 7,453 $ 7,602$ 7, :trtractor's Prolit Margin (^) $ 105,000 $ 107,1 00 $ 10s,242 6 11 1,427 $ 't't3,655 $ 1 15,928 $ 118.247 $ 120.
Statrng Salary D¡rect Cosls:
Facil¡ty ancl li4alerial Direct Costs:
Number of Beds (^40 40 40 40 40 40 40 ) Operat¡nq Pe¡ D¡em (^) $ 45.00 (^) $ 46.03 (^) $ 46.95 (^) $ 47.85 (^) s 48.71 (^) $ 45.42 (^) $ 50.82 (^) $ 5't.
Facilily Name Address C¡ty, State, Zip Code
STAFF]NG PLAN AND BUDGET JUSTIFICATION^ FORM REHABILITATION TREATME Tf SERyTCES - Phase I Adult Supportive Residential Facility BUDGET JUSTIFICATION
Exhibit J.l
may be utilized as needed to l¡st ANNUAL TREATMENT COSTS CATEGORY / ITEM FTEs Base Per¡od^ Period^3
Yeat 2 - FY21 Year 1 - FY
$ $ $^ s
s $
Number of Beds
Stafi¡ng Salary Direct Costs:
Fac¡lity and Mater¡al Direct Costs:
lndirect Costs:
TDCJ-PFCMOD Page^4 of^ l0^ Revised^812012018
696-PX'-19-P
Fac¡l¡ty Name Address C¡ty, State, Z¡p Code
BUDGET JUSTIFICATION
Note: Addìl¡onal ro$ are hidden and may be
CATEGORY / ITEM FTEs Base Peftod^2 Option Per¡od^3 Year 2 - FY I I I
Year 2 - FY I
Yea¡ 1 - FY I
Year 2 - FY I
Year 1 - FY I
Staffing Salary Direct Costs:
Fac¡l¡ty and Uaterial D¡rect Costs:
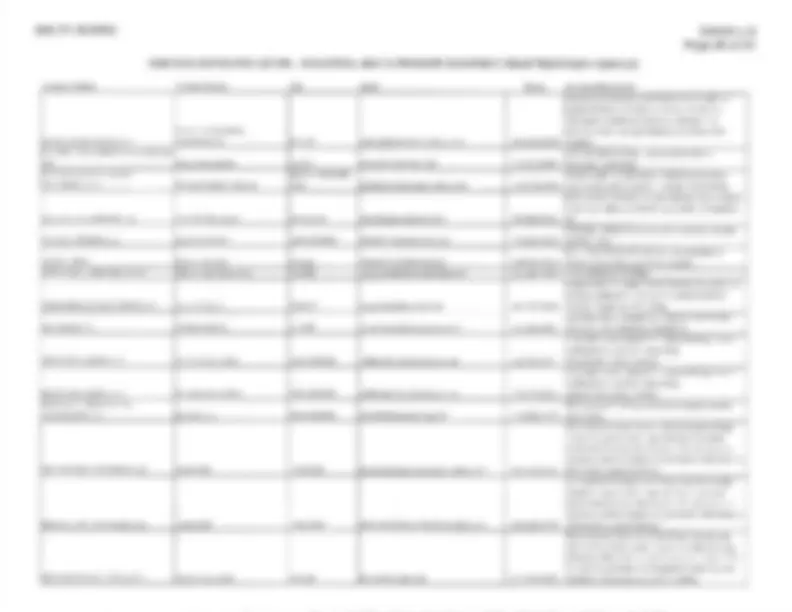
To be Completed for Phase l-B or Phase ll Adult Supportive Outpatient, TC lntensive Outpatient Relapse, and/or SACP Level ll Outpatient Facility
Please note this Staffing Plan is divided into two (2) sections. The first section, lndirect Staff, may include staffing positions associated with the Facility and/or Program, such as an Executive Director. The second section, Direct Staff, may include staffing positions assigned to the Facility and/or Program,
Facility Name:
Position Title:
Special Qualif ications:
Calculated (^) cells are locked and include the following: Total FTEs, Total lndirect Staff, Total Direct Staff, and Grand Total
ËXAMPå.H
Exhib¡t J.
REHABILITATION TREATMENT SERV/CES -^ Phase l-B or Phase Il Adult Supportive Outpatient, TC lntensive Outpatient Relapse, and/or SACP Levell ll Outpatient Facility
as needed to l¡st add¡tional infomãl¡on Position Titlê
Executive D¡rector
spec¡al Qualif¡cat¡ons
Bachelor Degree, 3 Yrs. Exp., ULM
Total HoursMleek
Total FTES
Business Manager 2 Yrs. College, 3 Yrs. Exp. 20.00 0. Receptionist HSGED, 2 Yrs. Exp. 40.00 1.
Program D¡rector LCDC, 10 Yrs Exp., ULM 40.00 1. lntake Coordinator HSGED, 3 Yrs. Exp. 40.00 1. Counælor LCDC 80.00 2.OO Counselor lntern LCDC-Ct 80.00 2.OO
GRAND TOTAL 320.00 8.
696-PX'-19-P
To be Completed for Phase l-B^ or^ Phase ll^ Adult^ Suppotfive Outpatient,^ TC^ lntensive Outpatient Relapse,^ and/or SACP Level ll Outpatient Facility
completed for each location.
Base Period and Option Period ln these columns, the estimated expenditures for each individual budget line item^ must be entered for the^ term^ of^ the Columns: Contract. Other Direct Costs: These are expenditures associated with the direct operation of the Facility, excluding salaries. lndirect Costs: These are expenditures associated^ with^ oversee¡ng^ the Contract,^ but not d¡rectly^ related^ to^ the^ Facility. Calculated cells are locked and include the following: Subtotals and Grand Totals.
qhtbl (^) J, STAFFING PLAN AND BUDGET JUSTIFICATION FORM
Address^ Facility Name City, State, Zip Code
CATEGORY / ITEM Dkector
FTEs
YEAT 1 - FYZU I$ 48.
feat z - tYzl I$ 48.960 I$ 49,
fea¡ 1 - t\¿ I$ 51,
Year 2 -FY I$ 52,
54,056 55,
Yeat 2 - FY2l I$ ntake Coord¡nator (^100) $ 20,000 20.400 $ 20.808 $ 21.224 $ 21.84ø $ 22.082 $ 22.523 22, lounselor 2.OO (^) $ 84,000 (^) $ 85,680 (^) $ 87,394 $ 89,141 $ 90,924 $ s2,743 û 94.598 $ s6, $
$
$
$ 93,
lntem 2.
$ 95,
$ 54,
$ 97,
$ 55,
$ s9,
$ 56,
$ 10't,
$
$ 1 LJtilities (^) $ 42,000 (^) $ 42,440 $ 43.697 s 44.571 $ 45,462 $ 48.371 $ 47.299 $ 48, Cffce Supplies (^) $ 2,500 (^) $ 2,550 (^) $ 2,601 (^) $ 2,653 (^) $ 2,706 (^) $ 2,760 $ $ 2, :uriculum (^) $ 1,500 $ 1,530 $ 1.561 (^) s 1.592 (^) $ 1.ø24 (^) $ 1,656 $ 1.689 (^) $ 1, $
50
$
$ 51
$ 2,
$
2,
54,
$
$
$ 2,
$ 55,
$ 2,
$ 56,
$ 2, EE-.= E r$ 57,
/ Fax l'rachine
Sãleries
2,O
lndirect Fr¡noe Benefits s 10.000 $ 10.200 s 't0,404^ $ '10.612^ $ 10,824 $ 11,041 $ 11,242 $ 11,
Stafflng Salary Direct costs:
Fac¡l¡ty BUOGET JUSTIFICATION Faoility Name Address
CATEGORY / ITEM FTEs Elase^ ter¡od^ Period Three
I I I
I
Year 1 - FY I
Yèat 2 - FYz'l I
Yea¡ 1 - FY I
YeaÍ 2 - FY Staff¡ng Salary D¡rect Costs I
Other D¡rect Costs (details requ¡red):
Enter your company's name here: Requisition#: 696-PF-'19-P
696-PF-19-P002 Exhibit^ J. e 2 Of 90 Rev^ 2t't
[[!reAÐ RespoNornls^ SUBcoNTRAcTNG^ INTENTToNS
a. (^) Check the appropriate box (Yes (^) or No) that identifies your (^) subcontracting intentions: {*. yes,^ I will be subcontracting portions of the contract. (lf Yes, complete ltem b of this SECTION and continue to ltem c of this SECTION.) f..^ lVo,^ I^ will not^ be^ subcontracting^ 4y portion^ of^ the contract, and^ I^ will^ be^ fulfilling the entire conhact with^ my^ own^ resources,^ including^ employees,^ goods,
Item # Subcontracting Opportunity 0escription
HUBs Non-HUBs Porcentage of the contract oxpscted to be subcontracled to HUBs with which you^ do (^) fot have a continuous contract* ¡n place
Percentage (^) of the contracl expected to be subcontracted to HUBs with which you have a continuous contracl* in^ place^ for more than five (5) vears.
Percentags of the contracl sxpected to be subcontracted to non.HUBs.
1 Yo o/^ o//o 2 Yo /o Yo 3 Yo ot^ o/o 4 o/o 5 10 to ot TO 6 to Yo Yo (^7) Yo Yo I Yo % I o/o^ % (^10) % o/o 11 Yo (^12) Yo Yo 13 to c/ 't4 10 o/o 15 Yo Yo Yo
c. (^) Check the appropriate box (Yes (^) or No) that indicates whether you will (^) be using onlv Texas certified HUBs to perform all of the subcontracting opportunities you listed in SECTION 2, ltem b. f.^ Yes (lf (^) Yes, continue to SECTION 4 and complete an "HSP (^) Good Faith Effort - (^) Method A (Attachment A)" for each of the subcontract¡ng opportunities you listed.) f -^ lVo^ (lf No,^ contlnue^ to^ ltem d, of^ this SECTION,)
f-.^ Yes (lf Yes, continue to SECTION 4 and complete an "HSP Good Faith Effort -^ Method A (Attachment A)" for each of the subcontracting oppofunities you listed. l..^ No (lf (^) tVo, continue to SECTION 4 and complete an "HSP Good Faith Effort - Method B (Attachment (^) B)" for each of the subcontracting opportunities you listed. *9gIliUgJtSJgI@Í: (^) Any existing written agreement (including any renewdls (^) that are exercised) between a prime contractor and a HUB vendor, where the HUB^ vendor^ provides the^ prime contractor with^ goods^ or^ servìce,toincludetransportationanddelivery^ under the^ same contract
the contract ís considered cont¡nuous. Two or more contracts that run concufiently or ovørlap one another for different periods^ of^ time^ are considered by CPA to be individual contacts rather than renewals or extensions to the original contract ln such situations the prime^ contractor and HUB vendor are enter¡ng (have entered) into (^) "new" contracts.
696-PF-í9-P002 Exhibit^ J. P e3of90 Rev.2h
EEEreEÐ 4.) Self^ Penf^ ORMlNc^ JUSTIFICATION^ (tf you responded "No"^ to^ SECTTON 2,^ ltEm^ a,^ you must^ complete^ this^ SECTIoN^ and^ continue^ to^ sEcTloN
supplies, materials and/or equipment.
documentation submitted with ihe HSP is true and conect. Respondent understands and agrees that, if^ awarded anv^ oortion of^ the^ reouisition:
. (^) The respondent will provide notice as soon as practical to all the subcontractors (HUBs and Non-HUBs) of their selection as a subcontractor for the awarded contract. The notice must specify at a minimum the contracting agency's name and its^ point^ of^ contact^ for the^ contract,^ the^ contract^ award^ number,^ the subconfacting opportunity they (the subcontractor) will perform, the approximate dollar value of the subcontracting opportunity and the expected percentage^ of
point of contact for the contract
. (^) The respondent must submit monthly compliance reports (Prime Contractor Progress Assessment Report (^) - PAR) to the contracting agency, verifying its compliance with the HSP, including the use of^ and^ expenditures^ made^ to^ its^ subcontractors^ (HUBs^ and^ Non-HUBs).^ (The^ PAR^ is^ available^ at httol/www.comptroller.texas.oov/purchasinqldoæ/hub-forms/ProqressAssæsmentReportForm.xls). o (^) The respondent must seek approval from the contracting agency prior (^) to making any modifications to its HSP, including the hiring of additional or different
respondent may be subject to any and all enforcement remedies available under the contract or othenruise available by law, up to and^ including debarment^ from^ all state contracting,
. (^) The respondent must, upon request, allow the contracting agency to perform on-site reviews of the company's headquarters and/or work-site where services are being performed^ and must provide^ documentation regarding^ stafüng and^ other ræources.
Reminder: Þ (^) tf you (^) responded "Yes" (^) to SECTION 2, ltems c or d, you must complete an "HSP^ Good Faith Effort - Method A (Attachment A)" for each of the subcontracting opportunities you^ listed in SECTION^ 2, ltem^ b, Þ tt you^ responded "No"^ SECTION 2, ltems c and d, you must complete an "HSP^ Good Faith Effort^ -^ Method^ B^ (Attachment B)"^ for each^ of^ the subcontracting opportunities you^ listed in SECTION 2, ltem b.
Date
Enter your company's name here:^ Requisition#: 696-PF-19-P
Enter your company's name here: Requisition#: 696-PF-19-P
696-PF-19-P002 Exhibit J. Page 5 of 90
HSP Good Faith Effort -^ Method B (Attachment^ B) (^) Rev. 2h
IMPORTANI: lf you responded "Âto" to SECTION 2, ltems c and d of the completed HSP form, you must submit a completed "HSP Good Faith Effort -
or download the form at http://www,comptroller,texas.qov/purchasinq/docs/hub-forms/hub-sbcont-þlan{fe-achm-b,ndf.
E¡llllul¡fl Su^ ecoNrRrcïNc^ OppoRruNrry Enter the item number and description of the subcontracting opportunity you listed in SECTION 2, ltem^ b,^ of the completed^ HSP^ form for which you^ are^ completing^ the attachment.
specific portion of work,
Check the appropriate box (Yes or No) that indicates whether you^ will be subcontracting the portion of work you^ listed in SECTION B-1 to your^ Protégé.
f* -^ Yes (lf Yes, continue to SECTION 84.) f -^ No^ / Not^ Applicable^ (lf^ lVo^ or^ Not Applicable,^ continue to SECTION B-3 and SECTION B-4.)
E[pTAEfl Nor^ ncnro¡r^ Or^ Su^ ecoNrRAcr^ Nc^ Opponrunrw
htto:/lwww.comptroller.texas.qovipurchasino/doæ/hub-forms/HUBSubcontractinq0ppodunitvNotificationForm.pdf.
Retain supporting documentation (i.e.,^ certified letter, fax, e-mail) demonstrating evidence of your good faith effort to notify the Texas^ certifìed HUBs^ and trade
trade organizations^ or development^ centers is^ considered to^ be "day^ zero"^ and does not count as one of the^ seven^ (7) working days.
specified a different time period, you must allow the HUBs at least seven í) workinq davs to respond to the notice prior^ to you submitting your bid^ response^ to the
Underutilized Business (HUB) Search directory located at http://mvcna.cpa.state.ü.us/toasscmblsearch/index.isp, HUB Status^ code^ "A"^ signifies^ that the^ company^ is a Texas certified HUB. b. List the three (3) Texas certified HUBs you notified regarding the subcontracting opportunity you listed in SECTION B-1. lnclude the company's Vendor lD (VlD) number, the date you (^) sent notice to that company, and indicate whether it was responsive or non+esponsive to your^ subcontracting opportunity notice.
Company Name (^) (0o not enter Texas VIDSocial Security t{umbere.}^ Date (mm/dd/yyyy)^ Notice Sent Did the HUB Respond? f -Yes^ f -No 1..-Yes f -No f -Yes {- -No c. Provide written notification of the subcontracting opportunity you listed in SECTION B-1 to two (2)^ or more hade organizations or development centers in Texas to
different time period, you must provide your subcontracting opportunity notice to trade organizations or development centers at least seven (l^ workino days prior to
subcontracting opportunities is available on the Statewide HUB Program's webpage at http://www.comptroller.texas.qov/purchasinq/vendor/hubhesources.php.. d. (^) Listtwo(2)tradeorganizationsordevelopmentcentersyounotifiedregardingthesubcontractingopportunityyoulistedinSECT|ONB-l.lncludethedatewhen you sent notice to it (^) and indicate if it accepted or rejected your notice.
Trade Organizations or Development Centers Date (mm/dd/yyw)^ Notice Sent Was the Notice Accepted? f" .Yes^ f- .No f* .Yes^ f -No
(Attachment (^) B)
696-PF-r9-P
HSP Good Faith Effort -^ Method B ttachment B
Exhibit J. Page 6 of 90
Cont. Rev.2h
[[[IU|UE[! Suecoȡrnrcron^ Selecroru Enter the item number and description of the subcontracting opportunity^ you^ listed in^ SECTION^ 2,^ ltem^ b,^ of the^ completed^ HSP form for^ which^ you are^ completing^ the attachment.
a. Enter the item number and description of the subcontracting opportunity for which you are completing this Attachment B continuation page.
expected percentage^ of work to be subcontracted. When searching for Texas certified HUBs and verifying their HUB status ensure that you^ use the State of^ Texas'
HUB status code "4" signifies that the company is a Texas certified HUB.
c. (^) lf any of the subcontractors you have selected to perform the subcontracting opportunity you listed in SECTION B-1 is p!^ a Texas certified HUB, provide^ written justification for your (^) selection process (attach (^) additional page if necessary):
REMINDERI As spæified in SECTION 4 of the completed HSP form, if you (resoondent) are awarded any portion of the^ requisition,^ you^ are^ required^ to^ provide notice as soon as practical^ to all the subcontractors^ (HUBs^ and^ Non-HUBs)^ of^ their^ selection^ as^ a^ subcontractor.^ The^ notice^ must specify^ at^ a^ minimum^ the
approximate dollar value^ of the subcontracting opportunity^ and^ the expected^ percentage^ of the total contract that^ the subcontracting opportunity repræents.^ A^ copy^ of^ the notice required by this section must also be provided to the contracting agency's point of contact for the contract no later than ten (10) working days^ after^ the^ contract is awarded.
(Attachment B)
Enter your company's name here:^ Requisition#:^ 696-PF-19-P
Company Name^ Texas^ certified^ HUB
Texas VID or fede¡al EIN Do not enter Social Security Numbers. Ityou do not know their VID I ElN, leave the¡r Mt / EIN t¡eld blenk.
Approximate DollarAmount
Expected Percentage of Contract f .yes (^) f .¡lo (^) $ o/o f -Yes^ f* _No^ $ o/o ¡ .Yes^ f .No^ $ o/n ¡ -Yes^ l- -No^ $ o/o ¡ -Yes^ f -No^ $ o/o ¡ .Yes^ f .No^ $ o/o f -Yes^ (^ -No^ $ Yo ¡ .Yes^ f^ .No^ $ o/o f.Yes a .No^ $ o/o ¡ .Yes^ f .No^ $ o/o
696-PF-19-P002 Exhibit^ J. Page 8 of 90
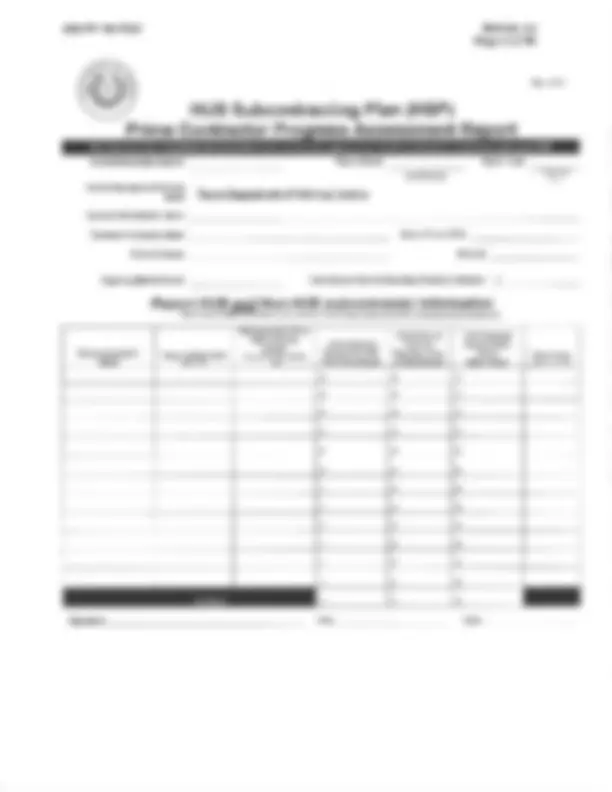
HUB Subcontracting Plan (HSP)
Contract/Requisition Number:
Prime Gontractor P
ress Assessment Re ort
(mm/dd/yyyy) (Agency Onty)^ Us
This form must be completed and submitted to the contracting agency each month to document compliance with^ your^ HSP
Name:
Contractor (Company)^ Name: Point of Contact:
Reporting (Month) Period
State of Texas VID #: Phone #:
Report HUB*Note: and Non-HUB subcontractor information Texas ceñ¡f,ed HUB status can be verified on^ llne^ at: hll,s;//mvcpa.cpa.stale.û.usftpasscmblsearch/index.isp
Subcontractor's
*Texas certified HUB?
Subcontractor's VID or HUB Certificate Number {Requlred lf TexasHTIBì^ cert¡f led
Total Contract $ Amount from HSP with Subcontractor
Total $ Amount Paid This Reporting Period to Subcontractor
Total Contract $ Amount Paid to Date to Subcontractor
Object Code lAoêncv Us Onlv) $ o^ $ $ $ $ $ $ $ $ $ $ $ $ $ $ o^ $
$ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $
Exhibit
J.
Page
of
asiancontractor@gmail.
com
rwashington@blackcontractors.orgchum@dbcc.orgconstruction@dfrvmsdc.
com
gquezada.gdhcc.
com
beverly@gtmbc. com
Exec-Admin@AustinAsianChamber.
org
nmc-@austinbcc.orgmiltonthibodeaux@gmail.
com
randymagdaleno@yahoo. comadmin@hcadesa.orgyolanda@regionalhca. orgmzarate@houstonhispanicchamber.
com
angela. freeman@hmsdc.
org
com
gmcdermott@uspaacc-sw. org^ asteele@wbcsouthvl'est.
org
bids@wbea-texas.orgdirector@womencontractors.
org
512-926-s4r0214485-0467214421-5510 214-637¿24r2r4-s20-t687 361-698-t024 9ts-566-97t4 817-332-6438 409-722-5402 s124s9-l
183
PHONE
18
I
10
MATLING
4201 Ed Bluestein
Street, Suite 251, Dallas,
Mafin
Jr.
Dallas,
Stemmons
5th
Suite 550,
Dallas,TX
Avenue,
Dallas,
Corpus
Paso,
South Freeway. Suite
2
1 1,
Fort
7
5064, Beaumont,
7 7 7
8001 Centre Park
Street, Suite
17071/2 South Post Oak
Houston,
Houston,
Avenue. Dallas,
Street, Suite 890, Houston.
Three
Suite 555, Houston,
3825 Dacoma St., Houston,
200 East Grayson, Suite 203,
San
912 Bastrop
410 Suite 230,
San
Street. Buda, Texas 78610
920 E. Dean Keeton,
TX
Sheet,
Suite
Houston,
ORGANIZATION
Contractor
Contractors Association
DallasÆort
Dallas
Chamber
Commerce
DFW
Supplier Development
Dallas Hispanic Chamber
Commerce
College
Corpus
Paso
Hispanic Chamber
Commerce
Fort
Chamber
Commerce
Golden Triangle
Business
Greater Asian Chamber
Commerce
Greater
Chamber
Contractors Association
Hispanic Contmctors Association
Hispanic Contractors Association
Regional
Houston Hispanic Chamber
Commerce
Houston
Supplier Development
Assoc.
Contractors
San
Hispanic Chamber
Commerce
Southwest
Supplier Development
Texas Assoc.
of
African
American
of
Commerce
of
Chambers
of
Commerce
Chamber
Commerce
U.S. Hispanic Contractors Association
de
Pan
Asian
Chamber
Commerce SW
Business
Southwest
Business Enterprise
Women Contractors Association