


Common asked questions about
ChEIs – Where is the answer?
Switching ChEIs – What is the
rationale?
How long does ChEls get
prescribed?
When to stop? What would happen
afterward?
When to do an ECG?
Docsity.com


Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Community
Ask the community for help and clear up your study doubts
Discover the best universities in your country according to Docsity users
Free resources
Download our free guides on studying techniques, anxiety management strategies, and thesis advice from Docsity tutors
An overview of commonly asked questions regarding cheis (cholinesterase inhibitors) including reasons for switching, indications, discontinuation, and results from various studies. Topics covered include intolerance, adverse events, and practical guidelines for discontinuation.
Typology: Slides
1 / 19

This page cannot be seen from the preview
Don't miss anything!
Pharmacological Properties of ChEIs
Cognitive and functional measure – dose response Behavioural manifestations – variable
Summary of the Studies
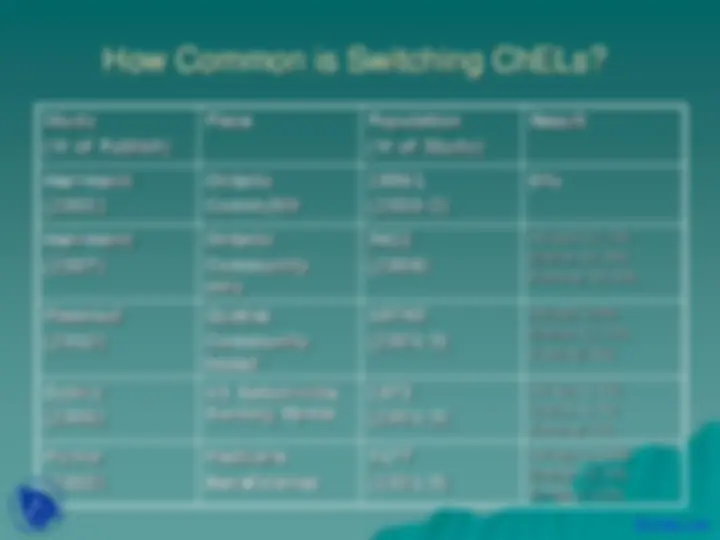
How Common is Switching ChELs?
Study (Yr of Publish)
Place Population (Yr of Study)
Result
Herrmann (2002)
Ontario Comm/NH
28961 (2000-2)
6%
Herrmann (2007)
Ontario Community only
5622 (2006)
Aricept 21.9% Exelon 32.3% Reminyl 32.3%
Massoud (2010)
Quebec Community based
18748 (2001-3)
Aricept 10% Exelon 11.7% Reminyl 5%
Dybicz (2006)
US Nationwide Nursing Home
2873 (2001-3)
Aricept 3.3% Exelon 4.7% Reminyl 2%
Mucha (2008)
Medicare Beneficiaries
3177 (2001-3)
Aricept 14.5% Exelon 21.5% Reminyl 15%
Discontinuing ChLs - Survey from C5R
Survey of Canadian Dementia Experts
Effectiveness
Survey Results (con’t)
Adverse Events
Others to consider
Practical Guidelines for Discontinuation
Ensure compliance and dose adjustments.
Concomitant medical conditions, such as delirium or depression, and the initiation of inappropriate drugs should be ruled out.
In the case of intolerance , switching to a second ChEI should not be tried before complete resolution of side-effects after discontinuation of the initial agent.*
The second ChEI can then be initiated at the usual starting dose and increased according to the recommended titration scheme, or titrate up more rapidly (two-week intervals) until the minimal therapeutic dose.
When considered for lack of benefit , switching ChEIs can be done overnight.
Switching for loss of benefit after taking the initial ChEI for several years is not suggested. Add Memantine.
Case Studies in ChEIs
What can be learnt from studies?
Incidence is very low.
Rarely, they cause or unmask
parasympathetically mediated bradycardia except in significant overdose.
People with SSS or other cardiac conduction
defects may be at a theoretically greater risk
Before beginning treatment with an AChE
inhibitor, it is necessary to:
If a patient on an AChE inhibitor presents with syncope, one should:
Cardiac conduction problems related
to AChE inhibitors: