Download PATHOLOGY AND MICROBIOLOGY and more Slides Pathology in PDF only on Docsity!
CHRONIC OBSTRUCTIVE
PULMONARY DISEASE
( COPD )
- COPD or chronic obstructive airway disease (COAD) are commonly used clinical terms for a group of pathological conditions in which there is chronic, partial or complete, obstruction to the airflow at any level from trachea to the smallest airways resulting in functional disability of the lungs i.e. these are diffuse lung diseases.
- One etiologic factor which is a common in all forms of COPD is smoking.
- The following diseases are included in COPD:
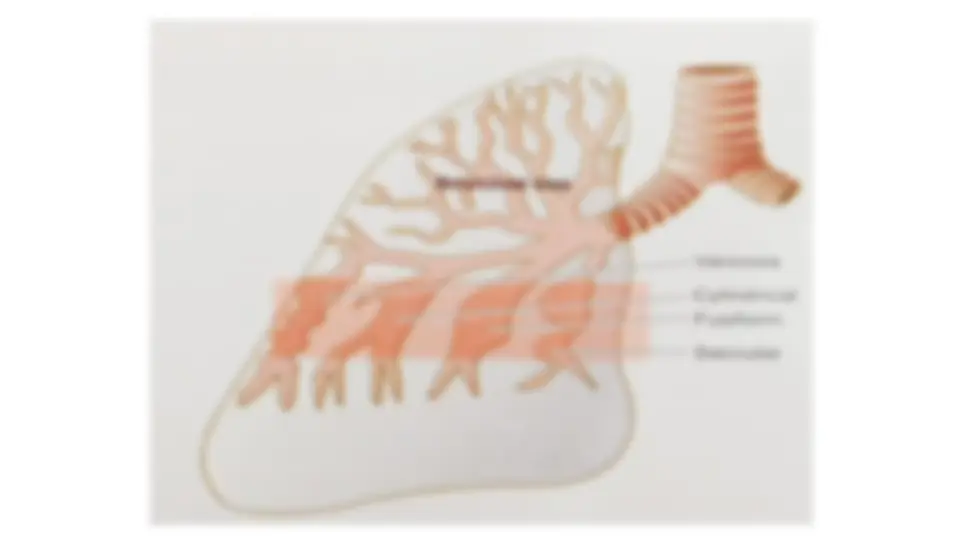
- I. Chronic bronchitis
- II. Emphysema
- III. Bronchial asthma
- IV. Bronchiectasis
- V. Small airways disease (bronchiolitis)
ETIOPATHOGENESIS
❑ Smoking The most commonly identified factor in causation of chronic bronchitis and in emphysema.
- Heavy cigarette smokers have 4 to 10 times higher proneness to develop chronic bronchitis.
- Prolonged cigarette smoking appears to act on the lungs in a number of ways:
- i) It impairs ciliary movement.
- ii) It inhibits the function of alveolar macrophages.
- iii) It leads to hypertrophy and hyperplasia of mucus-secreting glands.
- iv) It causes considerable obstruction of small airways.
- v) It stimulates the vagus and causes bronchoconstriction.
❑ Atmospheric pollution
- The incidence of chronic bronchitis is higher in industrialised urban areas where air is polluted.
- Some atmospheric pollutants which increase the risk of developing chronic bronchitis are sulfur dioxide, nitrogen dioxide, particulate dust and toxic fumes.
❑ Occupation
- Workers engaged in certain occupations such as in cotton mills (byssinosis), plastic factories etc. are exposed to various organic or inorganic dusts which contribute to disabling chronic bronchitis in such individuals.
❑ Infection
- Bacterial, viral and mycoplasmal infections do bronchitis.
- Cigarette smoke, predisposes to infection responsible for acute exacerbation in chronic bronchitis.
CLINICAL FEATURES
- There is overlap of clinical features of chronic bronchitis and pulmonary emphysema as quite often the two coexist.
- Persistent cough with copious expectoration of long duration; initially beginning in a heavy smoker with ‘morning catarrh’ or ‘throat clearing’ which worsens in winter.
- Recurrent respiratory infections are common.
- Dyspnoea is generally not prominent at rest but is more on exertion.
- Patients are called ‘blue bloaters’ due to cyanosis and oedema.
- Features of right heart failure (cor pulmonale) are common.
- Chest X-ray shows enlarged heart with prominent vessels.
- It is classified according to the portion of the acinus involved, into 5 types:
- centriacinar,
- panacinar (panlobular)
- para-septal (distal acinar)
- irregular (paracicatricial)
- mixed (unclassified) emphysema
ETIOPATHOGENESIS
- Th e association of the two conditions is principally linked to the common etiologic factors—most importantly tobacco smoke and air pollutants - protease-antiprotease hypothesis
- Protease-antiprotease hypothesis -1-antitrypsin (α-1-AT), also called 1-protease inhibitor (α -1-Pi), is a glycoprotein that forms the normal constituent of the α1-globulin fraction of the plasma proteins on serum electrophoresis
- It is normally synthesised in the liver and is distributed in the circulating blood, tissue fluids and macrophages.
- The normal function of α1-AT is to inhibit proteases and hence its name �1-protease inhibitor
- The proteases (mainly elastases) are derived from neutrophils.
- Neutrophil elastase has the capability of digesting lung parenchyma but is inhibited from doing so by anti-elastase effect of α1-AT.
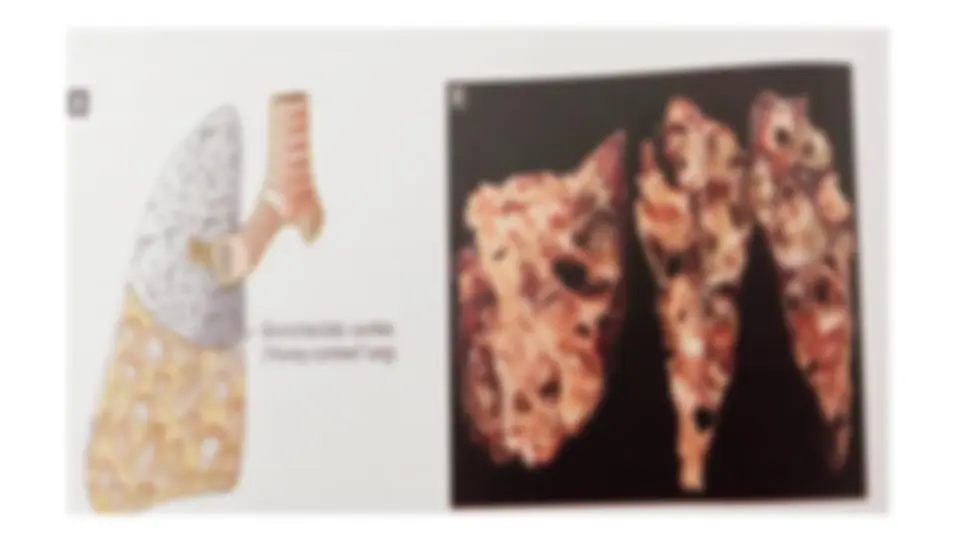
- Grossly, the lungs are voluminous, pale with little blood.
- The edges of the lungs are rounded.
- Mild cases show dilatation of air spaces visible with hand lens.
- Advanced cases show subpleural bullae and blebs bulging outwards from the surface of the lungs with rib markings between them.
- The bullae are air-filled cyst-like or bubble-like structures, larger than 1 cm in diameter.
- They are formed by the rupture of adjacent air spaces while blebs are the result of rupture of alveoli directly into the subpleural interstitial tissue and are the common cause of spontaneous pneumothorax
- Microscopically,
- depending upon the type of emphysema, there is dilatation of air spaces and destruction of septal walls of part of acinus involved i.e. respiratory bronchioles, alveolar ducts and alveolar sacs.
- Changes of bronchitis may be present.
- Bullae and blebs when present show fibrosis and chronic inflammation of the walls.
MORPHOLOGY OF TYPES OF EMPHYSEMA
• 1. CENTRIACINAR (CENTRILOBULAR) EMPHYSEMA
- Centriacinar or centrilobular emphysema is one of the common types.
- It is characterised by initial involvement of respiratory bronchioles i.e. the central or proximal part of the acinus
- This type of emphysema that usually coexists with chronic bronchitis and occurs predominantly in smokers and in coal miners’ pneumoconiosis - Grossly ,
- the lesions are more common and more severe in the upper lobes of the lungs
- characteristic appearance shows distended air spaces in the centre of the lobules.
- The lobules are separated from each other by fine fibrous tissue septa
- Large amount of black pigment is often present in the walls of emphysematous spaces
- In more severe cases, distal parts of acini are also involved and the appearance may closely resemble panacinar emphysema. - Microscopically,
- there is distension and destruction of the respiratory bronchiole in the centre of lobules
- The terminal bronchioles supplying the acini show chronic inflammation and are narrowed.
- Microscopically,
- usually all the alveoli within a lobule are affected to the same degree.
- All portions of acini are distended—respiratory bronchioles, alveolar ducts and alveoli, are all dilated and their walls stretched and thin.
- Ruptured alveolar walls and broken septa are seen between the adjacent alveoli.
• PARASEPTAL (DISTAL ACINAR) EMPHYSEMA
- It involves distal part of acinus while the proximal part is normal.
- This type is localised along the pleura and along the perilobular septa
- It is less often found in COPD but the common cause of spontaneous pneumothorax in young adults. - IRREGULAR (PARA-CICATRICIAL) EMPHYSEMA
- This is the most common form of emphysema, seen surrounding scars from any cause
- During life, irregular emphysema is often asymptomatic and may be only an incidental autopsy fi nding