Download NR511 Final Exam Study Guide(2022) and more Exams Nursing in PDF only on Docsity!
and
iextremities.
NR511 Final Exam
Study Guide
See Midterm and Week 1 Study Guide for content covering weeks 1, 2 & 3
Common Infections
- Impetigo
Impetigo iis ia isuperficial ibacterial iinfection iof ithe iskin. It is classified into
primary impetigo when there is a direct bacterial invasion of previously
normal skin or secondaryimpetigo when the infection arises at sites of minor
skin trauma. The occurrence of secondary impetigo is referred to as
impetiginization.
Impetigo iis imost ifrequently iobserved iin ichildren iages i 2 – 5 iyears iof iage,
although older children of any age and adults may also be affected. The
infection usually occurs in
warm, humid conditions and is i
i
Impetigo is i
minority of cases, either alone or in combination with
S. aureus. detected in some cases of impetigo.
causes
a is
Variants of impetigo include nonbullous impetigo, bullous impetigo, and ecthyma.
- Nonbullous impetigo—most common form of impetigo and begins as i
papules ithat iprogress ito ivesicles surrounded by erythema. Within a
week, the papules eventually become pustules that enlarge, break
down, and form thick, adherent
icrusts iwith ia icharacteristic igolden iappearance. iLesions iusually iinvolve ithe iface
i Regional lymphadenitis may occur, although systemic symptoms
are usually absent.
Occasionally,
iMRSA
primarily icaused iby iS. iaureus. iGroup iA
iStreptococcus i(GAS)
factors iinclude ipoverty, icrowding, ipoor ihygiene, iand
easily ispread iamong iindividuals iin iclose
icontact. iRisk
extend ithrough ithe iepidermis iand ideep iinto ithe
idermis.
- Bullous impetigo—Bullous impetigo is seen primarily in young children in which
the
, which later becomes
darker and ruptures, leaving a i
iaffected. Bullous impetigo in an adult with appropriate demographic
risk factors should prompt an investigation for previously undiagnosed human
immunodeficiency virus (HIV) infection.
- Ecthyma—This form of impetigo, caused by group A, beta-hemolytic
Streptococcus
(Streptococcus pyogenes), consists
of an i i
Ecthyma iresembles
i
margins
covered with yellow crust surrounded by raised
violaceous
"punched-out"
iulcers
ulcerative iform iin iwhich ithe
ilesions
iThe itrunk iis imore
ifrequently
thin ibrown
icrust.
ivesicles ienlarge ito iform iflaccid ibullae iwith iclear
iyellow ifluid
ithermal iburn. This serious infection is more commonly seen in children and
usually begins in the intertriginous areas.
si treptococci i(groups iA, iB, iC, iG, iand iF), iand iS. iaureus i(gram i+)
The imost icommon iare ibeta-hemolytic
- Cellulitis
Cellulitis is an acute infection as a result of bacterial entry via breaches in
the skin barrier. As the bacteria enter the subcutaneous tissues, their toxins
are released whichcauses an inflammatory response.
✓ Cellulitis and erysipelas is almost always a unilateral infection
with the most common site of infection being the lower
extremities.
✓ Cellulitis involves the deeper dermis and subcutaneous fat.
adults.
✓ The vast majority of pathogens associated with cellulitis are
from either Streptococcus or Staphlococcus bacteria. i
✓ Both erysipelas and cellulitis manifest with areas of skin erythema,
edema, warmth and pain. Fever may be present. Additional
manifestations of cellulitis and erysipelas include lymphangitis and
inflammation of regional lymph nodes. Edema surrounding the hair
follicles may lead to dimpling in the skin, creating an appearance
reminiscent of an orange peel texture called "peau id'orange".
✓ Cellulitis may present with or without purulence
✓ patients with cellulitis tend to have a more indolent course with
development of localized symptoms over a few days.
✓ Many patients with cellulitis have underlying such as tinea pedis,
lymphedema, and chronic venous insufficiency. In such patients,
treatment should be directed at both the infection and the
predisposing condition if modifiable.
✓ Patients with cellulitis or erysipelas in the absence of abscess or
purulent drainage should be managed with empiric antibiotic
therapy. Patients with drainable abscess should undergo incision
and drainage.
➢ should be managed with empiric therapy for infection due to beta-
hemolytic streptococci and methicillin-susceptible Staphylococcus
aureus (MSSA) with:
- Cephalexin 500 mg four times daily (alternative for mild penicillin allergy)
- Clindamycin 300 mg to 450 mg four times daily (alternative for
severe penicillin allergy)
➢ Good choices for uncomplicated cases of cellulitis that are not
associated with human or animal bites include dicloxacillin or
cephalexin for 10 to 14 days.
➢ If pt has severe PCN allergy rx erythromycin
➢ If caused by animal or human bite: amoxicillin-clavulanic acid
(augmentin) for 2 weeks
The coverage for MRSA is achieved by adding to amoxicillin one of the
following: Bactrim DS twice daily
Doxycycline 100 mg twice daily
Minocycline 200 mg orally once, then 100 mg orally every 12 hoursIf
clindamycin is used, no additional MRSA coverage is needed.
I. Describe ian iappropriate iempiric iantibiotic itreatment iplan
ifor icellulitis
Cellulitis iis iobserved imost ifrequently iamong imiddle-aged iindividuals
iand iolder
b. Periorbital cellulitis d. "Flesh-eating" cellulitis
following
icircumstances.
Prophylactic iantibiotics iare iadministered ito ipatients iwho
ipresent ifor
- Necrotizing fasciitis
Considered as a severe case of cellulitis must refer to ER, can be a
differential diagnosis of cellulitis
Defined as deep infection that results in progressive destruction of the
muscle fascia. The affected area may be erythematous, swollen, warm, and
exquisitely tender. Pain outof proportion to exam findings may be observed.
✓ The hallmark of this infection is its rapid progression and the severity
of the symptoms. The progress of the infection is measured in terms
of hours instead of days, and the border can be seen to literally
spread in just a few hours.
✓ This infection is caused by “flesh-eating bacteria,” and loss of life
or limb is a potential complication.
Quiz: Mark has necrotizing fasciitis of his left lower extremity. Pressure on the
skin reveals crepitus due to gas production by which anaerobic bacteria?
a. Staphylococcal aureus c. S. pyrogenes
d. Streptococcus
- Mammalian bites
Soft tissue trauma caused by animal and human bites have serious clinical
implications because of the potential for complications.
Bite wounds should be irrigated copiously with sterile saline, and grossly
visible debris should be removed. i
i
i
- Deep puncture wounds (especially due to cat bites)
- Wounds requiring surgical repair
- Moderate to severe wounds with associated crush injury
- Wounds in areas of underlying venous and/or lymphatic compromise
- Wounds in immunocompromised hosts
Amoxicillin/clavulanate i 875 img/125 img itwice idaily iis ithe iagent iof ichoice.
Alternative antibiotics include one of the following agents with activity
against Pasteurella.
- Doxycycline 100 mg twice daily
- Bactrim DS twice daily
- Penicillin VK 500 mg four times daily
- Ciprofloxacin 500 mg twice daily
Plus one of the following agents with anaerobic activity.
- Metronidazole 500 mg three times daily
- Clindamycin 450 mg three times daily
First-generation cephalosporins and macrolides should be avoided. The
duration of prophylactic oral antibiotics is 3–5 days, with close follow-up.
Tetanus toxoid should be given to those who have completed a primary
immunization series but who received the most recent booster 5 or more
years ago.
i iWounds ion ithe iface ior iin ithe
igenital iarea
Wounds ion ithe ihand(s) ior iin iclose iproximity ito ia
ibone ior ijoint
evaluation iof ia ibite iwound iwho ido inot iyet ihave isigns ior isymptoms iof
iinfection iin ithe
b. iClostridium
iperfringens
A i 24 - hour iurine iwith
Gross ipainless
glomerulonephritis), or nephrolithiasis; family history (e.g., of polycystic
kidney disease); and recent travel (potential exposure to parasitic
infections). i
2. Incontinence & overactive bladder - Urinary incontinence (UI) is the involuntary loss of urine from the bladder.
Incontinence is so frequent in women that many consider it normal.
Incontinence is also common in older men as a result of an enlarging
prostate. Incontinence can affect a person’s quality of life and may be
psychologically devastating.
a. Stress: Failure to store due to hypermobility of bladder neck,
intrinsic sphincter deficiency, neurogenic sphincter deficiency
Medications: Sedatives, hypnotics, antispasmodics
b. Urge: Failure to store due to urinary tract infection; vaginitis;
bladder stones and tumors; cortical, subcortical, and suprasacral
lesions; cerebrovascular accident; dementia; multiple sclerosis;
Parkinson’s disease; spinal cord transection Medications: Diuretics,
narcotics
c. Overflow: Failure to empty due to underactive detrusor, outlet
obstruction, diabetes mellitus Medications: Anticholinergics,
disopyramide, antihistamines, calcium channel blockers
d. Functional: Delirium, fecal impaction, manual dexterity and
immobility Medications: diuretics, hypnotics, alcohol, narcotics,
decongestants
Rx: Anticholinergic/Antispasmodic Agents: ex: tolterodine (Detrol LA) or
oxybutynin (Ditropan XL) for urge, overactive bladder and stress
incontinence. Contraindications: Closed-angle glaucoma, Myasthenia
gravis.
- Tricyclic Antidepressants: Imipramine (Tofranil) amitriptyline (Elavil) for OAB
and Urge incontinence
- The term overactive bladder (OAB) is often used interchangeably with the
term urge incontinence; however, they are different conditions. OAB is a
syndrome of symptoms that include urgency, frequency, and nocturia, all of
which are associated with involuntary contractions of the detrusor muscle.
Urge incontinence may or may not be a feature of this syndrome; about
one-third have urge incontinence.
3. Proteinuria - Proteinuria is usually indicative of a renal pathology, most often of
glomerular origin. Proteinuria can be functional as a result of acute illness,
emotional stress, or excessive exercise and is a benign process. It can also
develop from overproduction of filterable plasma proteins, especially
iBence iJones iproteins iassociated iwith imultiple imyeloma
- The most accurate way to quantify the amount of protein in the urine is a
24-hour urine collection; however, a spot urine albumin to urine creatinine
ratio can be measured and is a close approximation of the 24-hour urine
measurement. i
ia icardinal isymptom iof icertain imalignancies isuch ias
ibladder icancer.
l and corresponds to an excretion of less than 200 mg/dL
of protein.
- Causes of benign, or functional, proteinuria include orthostatic
proteinuria, exercise,
environmental conditions, fever, and acute illnesses. Orthostatic proteinuria occurs
when
iis
inorma
iindicative iof ia inephrotic iproblem. iA iurine ialbumin ito iurine icreatinine iratio
iof iless ithan i
ithan i 165 img iof iprotein iis iconsidered iabnormal iand ia ispecimen iwith imore
ithan i3. 5 ig iis
- Type of upper urinary infection: renal pelvis, tubules, or interstitial
tissue; may be unilateral or bilateral.
Risk factors: -female sex - indwelling catheter
-urinary tract obstruction - VUR
- Common pathogens: E coli, proteus, and Enterobacter (common in bowel flora)
- Acute pyelonephritis usually unilaterally
- S/S: - WBC in urine -WBC cast
- leukocytosis (inc WBC in blood)- fever
- N/V, chills - flank pain at cosovertebral
angle Dx: urinalysis: positive for bacteria, proteinuria, leukocyte
esterase, urinary nitrites,
hematuria, pyuria, and specifically white blood cell (WBC) casts (reflecting
the passage of neutrophils through the renal tubules)
Urine Cx: demonstrates greater than 100,000 cfu/mL, allowing for
identification of the causative organism.
-Tx: abx and hydration
First-line therapy ciprofloxacin (Cipro) 500 mg two times daily for 7 days, or
levofloxacin (Levaquin) 750 mg daily for 5 days.
In second-line therapy, trimethoprim-sulfamethoxazole (TMP-SMX) (Bactrim
DS, Septra DS) taken orally for 14 days may be as effective as amoxicillin-
clavulanate for 14 days in young women with their first pyelonephritis and
without anatomical abnormalities. However, given the prevalence of
sulfonamide and ampicillin resistance among common uropathogens, TMP-
SMX and amoxicillin are likely to be ineffective in cases of recurrent or moderate to
severe pyelonephritis (except in cases of Enterococcus infection, which calls for
the addition of amoxicillin [Amoxil] 500 mg PO three times daily).
Nitrofurantoin should be avoided because it does not achieve adequate tissue
levels.
Other effective choices are third generation cephalosporins (e.g., cefixime,
cefpodoxime, ceftriaxone), aminoglycosides (e.g., gentamicin, tobramycin),
or aztreonam, with fluoroquinolones reserved for antibiotic-resistant
organisms, hence the critical need for early urine culture to guide
pharmacotherapy.
6. Urethritis - Infections of the lower urinary tract can occur in the urethra, bladder,
and prostate. Infection of the urethra (urethritis) and infection of the
urinary bladder (cystitis) usually occur together.
- Common causes: E. coli, chlamydia or gonorrhea, trichomonas, HSV
- Pus in the urine is indicative of bacterial infection, such as cystitis,
urethritis, or prostatitis.
- Suprapubic tenderness is indicative of a bladder etiology, whereas
urethral discharge indicates a urethritis.
- Acute cystitis and urethritis produce gross hematuria and are more common in
women.
- Hematuria is also often present in lower and upper UTI, but not in vaginitis or
urethritis.
- Urethritis in men is rare; if left untreated or treated inadequately, it can
lead to complications such as urethral strictures, periurethral abscess,
urethral diverticuli, and fissures.
- Vaginal discharge in women and urethral discharge in men may suggest
sexually transmitted diseases (STDs). iPurulent iurethral idischarge
i(Neisseria igonorrhoeae) ior
receiving
estrogen
replaceme
n t
therapy
Genital
herpes
Dysuria,
fever,
headache,
myalgias,
neckipain,
vulvar pain,
photophobia
Sexually
active;
may have
vaginal
discharge
Grouped
vesicles
usually on
cervix or pubic
area, butm i
ay be vaginal;
tender inguinal
adenopathy
Viral
culture
optional
Urethritis Usually History of No suprapubic Urethral swab
asymptomatic; unprotected pain unless positive for
if symptoms sexual associated with white blood
develop, they exposure pelvic cells; obtain
are usually inflammatory Gram stain to
delayed (>1 disease; rarely, detect
week) visible urethral intracellular
discharge gram-negative
diplococci and
DNA probe for
Chlamydia and
gonorrhea
7. Renal calculi - Forms when solid in urine precipitate and is crystalized, due to
dehydration or increased in solutes
- Calcium oxalate and calcium phosphate stones account for 65% to 85% of
all cases of renal calculi.
Most common causes:
1. Calcium oxalate (forms in acidic urine) black to dark brown stone,
radiopaque on X- ray (white spot )Most common in men*
- Risk factors hyperoxaluria: - genetic defect: increase in oxalate excretion
- defect in liver metabolism
- diet heavy on oxalate rich foods: rhubarb, spinach, chocolate, nuts and beer
- Calcium phosphate (forms in alkaline urine) dirty white stone,
also seen as radiopaque on X-ray)
Risk factors hypercalcemia Risk factors hypercalciuria
Increased absorption in GI tract impaired renal tubular
reabsorption Hormonal causes like primary hyperparathyroidism
Low calcium diet: increased oxaluria due to less oxalate bound to calcium in GI tract
- vasectomy
- hypertension
- Lasix
- Uric acid stones (red-brown radiolucent on X-ray; transparent to X-ray)
the itriad iof
iflank
D) iAll iof ithe
iabove
- consuming lots of prurines which have high levels of uric acid
causing also gouty arthritis. Foods: shellfish, anchovies, red meat,
organ meat
Quiz: The clinician should question the patient with suspected gout
about use of which of these medications that may be a risk factor?
Low-dose aspirin
Thiazide diuretics
Ethambutol (abx for TB tx)
4. Struvite Stones (infection stones, dirty white and radiopaque on X-
ray) *** Most common in women**
- caused by bacteria, leading to urease then urea combined with CO
making urine alkaline
- Risk factors UTI, VUR, obstructive uropathies
- Cystine Stones (yellow or light pink, radiopaque on X-ray)
- Xanthine Stones (red-brown, radiolucent on X-ray) 8. Urinary tract cancer
- Gross painless hematuria is a cardinal symptom of certain
malignancies such as bladder cancer.
- in a UA glucose and protein positive
- Renal tumors are responsible for approximately 3% of all adult
malignancies. The incidence is higher in men (although the difference in incidence
has been decreasing over time), with onset between ages 55 and 70 years and
rarely occurring in people younger than 35 years of age. These cancers are curable
in more than 90% of patients if they are superficial and/or localized in the renal
pelvis or ureter. Tumors that are invasive have a 10% to 15% chance of being
cured. In children, inephroblastoma i(Wilms’ itumor) is common, comprising 5 % of
primary tumors, whereas sickle cell disease has a known, albeit rare, association
with carcinoma of the renal medulla.
- Cigarette smoking has a 25% to 30% correlation with the development of renal cell
carcinoma.
- Early signs of tumor growth are silent: Approximately 60% of the time,
patients present with gross ihematuria ias ithe ionly isymptom. The patient
complains of a dull, achy flank pain or abdominal mass in approximately 30%
of cases. In 10% to 15% of patients,
i
idisease.
- Tx: Treatment for a renal neoplasm is primarily surgical with a partial or total
nephrectomy, chemotherapy is not effective with this type of cancer; however,
immunotherapy using lymphokine-activated killer cells with or without interleukin-
2 may be helpful for selected patients. Radiation therapy is controversial but may
be used in combination with nephrectomy or for palliative effects in patients with
bone metastasis.
MaleComplain
ts
1. Testicular torsion
pain, ihematuria, iand iabdominal imass iis ifound, iwhich iis ioften ia isign iof
iadvanced
Obstructiveisymptomsiinclud
e
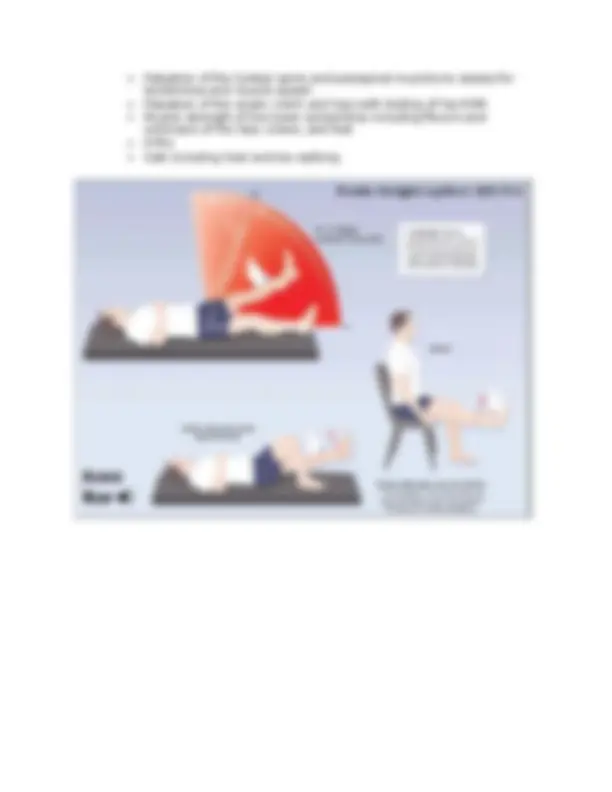
In the ER, manual reduction of the testis is usually performed and if not successful will be followed by
surgical exploration and may require removal of a nonviable testis.
Viability of the testicle is directly related to the duration of torsion, so again, time is of the essence. If
torsion occurred more than 6 hours prior, the likelihood of viability falls to 10–15%. Beyond 24 hours,
the viability rate falls below 10%. There is also a reduced rate of sperm production in patients who have
had torsion, whereby reproduction may be affected.
2. Benign Prostatic Hyperplasia
The prostate gland, is a walnut size gland positioned at the base of the bladder and in front of the rectum
that begins to enlarge as a man ages. It surrounds the urethra and as the prostate gets larger, it can
squeeze or partly cause obstruction. BPH is the common name for nodular hyperplasia and is one of the
most common conditions affecting men >40yrs old. As many as 50% of men experience symptoms of
enlarged prostate by age 60 and 90% of men will report symptoms by age 85
The causes of BPH are not fully understood. Aging is a risk factor and genetic predisposition may play a
role. Androgens are thought to play a key role. There has been no concrete evidence that diet,
environment, or sexual practices increase the risk for developing BPH. Obesity though does increase the
risk of development.
Symptoms of BPH usually involve a combination of obstructive and irritative voiding complaints. BPH is
not life-threatening but it is life altering. It is important to note that symptoms are not specific to BPH
(since many conditions result in an overlap of symptoms) so a complete work-up needs to be
completed.
Irritativeisymptomsiinclud
e
urinaryiretention
inabilityitoivoluntarilyistopitheiurineistream
overflowiincontinence
sensationiofiincompleteibladderiemptying
postvoididribbling
urinaryiurgency
urinaryifrequency
- hesitancy
- straining
- nocturia
- dysuria
DRE is done to determine the size of the prostate gland.
ienlarged. If the prostate is nodular or unusually firm, cancer should be suspected. Also, the size of the
prostate does not correlate with the severity of symptoms.
Quiz: During a digital rectal exam (DRE) on a 75-year-old man, the clinician suspects the patient has
prostate cancer. What physical finding should make the clinician suspicious? iAnienlargedirubberyigland
The DDx for BPH is extensive but the diagnoses can be categorized into 1 of the 3 following types:
- bladder outlet obstruction (cancer, stricture, bladderneckcontracture),
- nonobstructiveetiologies (neurogenic bladder, DM, Parkinson’s, Medications)
- irritative symptoms (neoplasm, bladdercancer, prostatitis, uti)
Diagnostic testing
- urinalysis and urine C&S is done to exclude infection and hematuria
- PSA is done to assess for prostate cancer
- urine cytology is done to exclude bladder cancer
- the AUA no longer recommends a serum creatinine on the initial evaluation should be done on
subsequent visits or if obstructive uropathy is present.
Keep in mind that there may be an elevation in the PSA in BPH just as it occurs in cancer so the PSA is
NOT diagnostic of either.
More advanced diagnostics include, should be done by an urologist:
- urodynamic studies to identify difficulties in emptying the bladder
- post-void residual urine test (PVR)
- cystoscopy
The iprostate iiniBPH iis iusually ismooth
iand
urgeiincontinence
decreasedistream