Download Critical Care Exam 2 Guide and more Exams Nursing in PDF only on Docsity!
Critical Care
Exam 2
Guide.Latest
Update.2024 Top
Ranked.
Trauma
· Trauma - caused by injury or external force
o 3 types
▪ Blunt
· Most common type
· When something hits the body. Ex. Car accidents, falls, beatings.
· Problem: Is you don’t always see the extent of the injury. Don’t know what’s
going on under the surface.
· FAST Scan (Focused Assessment with Sonography for Trauma)
o Quick ultrasound of organs in the abdomen to determine any internal injuries
· Abdominal injury most commonly associated with blunt forced trauma.
▪ Penetrating
· Anything that penetrates the body. Ex. Gunshot, stabbing, anything that
piercing the skin and is sticking out of you, ice picks. Less Common.
· 2 Problems:
o High infection risk. Especially with injuries to the abdomen.
o Did object hit any vital/internal organs?
▪ Depending on what organ is hit it can leak into the body (i.e
stomach/GI con- tents). We look at this when someone gets
shot. Did it hit anything vital?
▪ Blasts
· 3 concerns
o What got blasted? What kind of shrapnel what is exploding? Anything that
explodes.
o Injury to internal hollow organ from shockwaves. Depends on how
close you are to the blast. What is blasted out of the bomb maybe a
chemical or object ex: screws
o First concern : Whatever is being blasted out, chemicals from the bomb.
Second con- cern: Trauma to our hollow internal organs from the shock
waves. Final Concern: Sec- ondary injuries related to how close you
were to the blast. Ex: Could be thrown a distance injuring spinal cord.
o Secondary (tertiary) injuries (Blunt, head, spinal cord, burns, bleeding)
Triage
· Means to sort – based on the need of each patient.
· Any time you have multiple people in a large trauma. We triage patients by color.
· Color coding system
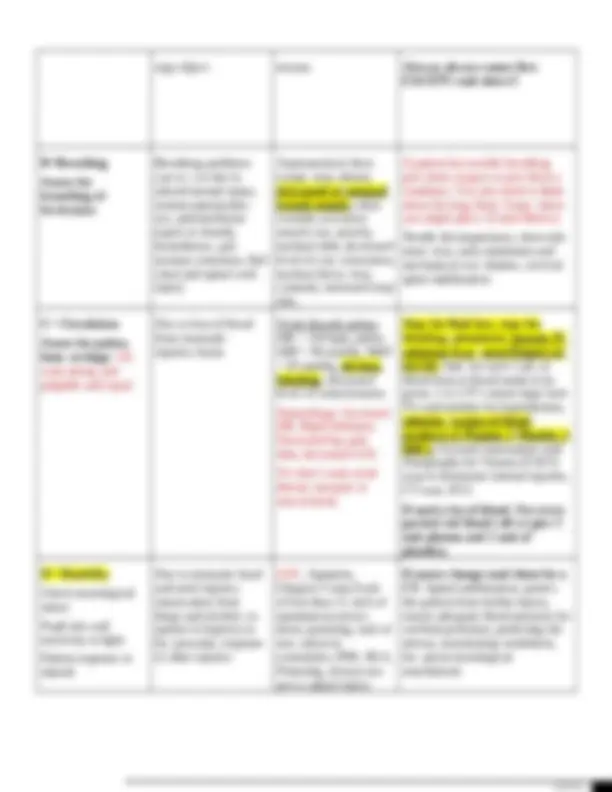
Findings
A=Airway – is our
pa- tient airways
intact if so move on
to B, if not per-
form an
intervention.
Assess airway
patency
Obstructions can occur
due to edema, posterior
dis- placement of the
tongue, in- ability to
protect airway due to
neurological
impairment or high
level spinal cord in-
jury, vomit, blood or a
for-
Shallow, noisy
breathing, stridor ,
central cyanosis, nasal
flaring, accessory mus-
cle use, anxiety,
inability to speak or
swallow, drooling,
decreased level of con-
sciousness , facial/head
First: Opening the airway with
a head- tilt-chin-lift or jaw-
thrust maneuver
Insertion of an oral or nasal
airway Endotracheal
intubation Tracheostomy of
crycoidthyrotomy
eign object trauma Airway always comes first
EXCEPT read above!!
B=Breathing
Assess for
breathing ef-
fectiveness
Breathing problems
can oc- cur due to
altered mental status,
tension pneumotho-
rax, pneumothorax
(open or closed),
hemothorax, pul-
monary contusion, flail
chest and spinal cord
injury
Asymmetrical chest
expan- sion, absent,
decreased or unequal
breath sounds, chest
wounds, accessory
muscle use, anxiety,
tracheal shift, decreased
level of con- sciousness,
tracheal devia- tion,
cyanosis, increased resp
rate,
If patient has trouble breathing
give them oxygen or give them a
ventilator. You also need to think
about the lung them. Some- times
you might place: (Listed Below)
Needle decompression, chest tube
inser- tion, early intubation and
mechanical ven- tilation, cervical
spine stabilization
C= Circulation
Assess for pulses,
hem- orrhage. We
want strong and
palpable and equal.
Due to loss of blood
from traumatic
injuries, burns
Weak thready pulses,
HR > 120 bpm, pallor,
SBP < 90 mmHg, MAP
< 65 mmHg, obvious
bleeding , decreased
level of consciousness
Hemorrhage: Increased
HR, Rigid abdomen,
Decreased bp, pale
skin, decreased LOC
We don’t want weak
thread, unequal, or
non-existent.
Stop the fluid loss, stop the
bleeding, administer isotonic IV
solutions (Lac- tated Ringers or
0.9 NS; 3mL for each 1 mL of
blood lost) or blood needs to be
given, 1 to 2 IV’s insert large bore
IVs and monitor for hypothermia,
adminis- tration of blood
products (1 Plasma: 1 Platelet: 1
RBC), Focused Assessment with
Sonography for Trauma (FAST)
scan to determine internal injuries,
CT scan, ECG
If need a lot of blood: For every
packed red blood cell we give 1
unit plasma and 1 unit of
platelets.
D= Disability
Check neurological
status
Pupil size and
reactivity to light
Patient response to
stimuli
Due to traumatic head
and neck injuries,
intoxication from
drugs and alcohol, re-
sponse to hypoxia or
hy- poxemia, response
to other injuries
LOC, Agitation,
Glasgow Coma Scale
of less than 11, lack of
spontaneous move-
ment, posturing, lack of
sen- sation in
extremities, PER- RLA,
Posturing, always sus-
pect a spinal injury.
If neuro change send them for a
CT. Spinal stabilization, protect
the patient from further injury,
ensure adequate blood pressure for
cerebral perfusion, protecting the
airway, maximizing ventilation,
fre- quent neurological
assessments
G= Give comfort
mea- sures
Trauma is both
physically and
emotionally painful
Pain, Anxiety, Grief,
Fear,
nonpharmacological
Ex: someone from
pastoral care sitting
with patient.
Provide emotional reassurance,
adminis- ter narcotics/antianxiety
as needed, pro- vide therapeutic
touch, family present, pastoral
care.
H= History
Obtain a complete
history and physical
as long as the patient
is stable. Head to toe
Assessment.
Need to determine the
cause to determine
possible in- juries
Evidence of abnormal
find- ings from
injuries
Perform a head to toe assessment,
obtain a history of the events as
well as the pa- tient’s past
medical history
I= Inspect
Posterior
Surfaces
Log roll the patient
to in- spect the back
etc.
To determine if there
are in- juries to the
posterior side
Evidence of abrasions,
ec- chymosis, wounds,
crepitus fractures,
edema, pressure ulcers
Log roll the patient and maintain
spinal immobility.
Trauma Injuries
Injury Clinical Manifestations Treatment
Tension Pneumothorax Severe respiratory distress,
chest pain, increased
respirations, hypoten- sion,
tachycardia, absent breath
sounds, tracheal deviation ,
cyanosis. Air is getting trapped
and cannot escape.
Prepare for needle decompression first and
then chest tube insertion.
The bio-physician will do this procedure.
Pneumothorax Severe respiratory distress,
chest pain, hypotension,
tachycardia, ab- sent breath
sounds, Air can escape.
Prepare for chest tube insertion
Dry suction, no bubbling, bubbles =
air leak Water seal, bubbling
Tube comes out use occlusive
dressing Never clamp chest tube,
only done by doctor
Open Chest Wound Severe respiratory distress,
chest pain, hypotension,
tachycardia, ab- sent breath
sounds
Seal the wound with an occlusive
dressing and tape on three sides (So air
can get back, if you tape on all 4 sides
patient can get a tension pneu-
mothorax. Prepare for chest tube
insertion.
Massive Hemothorax – blood
in the lung cavity
Decreased breath sounds,
dullness to percussion on the
affected side, hy- potension,
and respiratory distress
Prepare for blood transfusions, type and
crossmatch, IV insertion, prepare for chest
tube insertion
Pulmonary Contusion –
bruise in lung. That part of the
lung will not be able to
participate in gas ex- change
and that part of the lung that
becomes bruised will become
stiff. High risk then for
Chest wall abrasions,
ecchymosis,
bloody
secretions, decreased PaO 2
bruise of the lung. Bruised
part will not participate in gas
exchange, lung becomes stiff
Prepare for early intubation and
mechanical ventila- tion early. -
Spinal Cord Injury Decreased or absent movement
and/or sensation below the
level of injury.
Might see changes in breathing.
Observe ventilator effort, maintain spinal
immobiliza- tion, monitor motor and sensory
function, monitor for neurogenic shock
Decreased Level of
Consciousness
Mental status changes and GCS
of less than 11
Position the head midline and keep the head
of the bed elevated to prevent an increase in
intracranial pressure, prepare for CT scan,
aspiration precautions, intubation and
mechanical ventilation
Cardiac Tamponade: Fluid
around the heart.
Hypotension, muffled heart
sounds, and elevated venous
pressure (JVD) these are
known as Beck’sTriad
Prepare for a pericardiocentesis
Cardiac Contusion Bruise
of the heart.
Dysrhythmias, signs of blunt
chest in- jury, bruise to the
heart, presents like someone
who is having an MI, changes in
heart rate and bp, increased
cardiac enzymes. (troponin, CK
– MB)
Monitor for dysrhythmias, check cardiac
enzymes, in- otropic agents, O2 – treat like
an MI
Aortic Disruption also
known as aortic dissection. If
a patient has that and lives
they need surgery.
Weak femoral pulses,
dysphagia, hoarseness,
dyspnea and pain. Chest X-
ray will demonstrate a wide
medi- astinum, tracheal
deviation, rib frac- tures
Aortic dissection – tear in wall
of artery creating a false lumen,
weaken- ing of arterial wall.
No manifestations until rupture.
Prepare the patient for the OR for repair of the
aorta
Gastric and bowel injuries Abdominal pain, rigid abdomen,
absent bowel sounds or
decreased. Bowel has high
infection rate.
Surgical intervention.
Liver Injuries Right upper quadrant pain,
ecchymo- sis, hypotension,
rigid abdomen, can cause
hemorrhage.
Will complain of abdominal
pain.
Minor injuries are treated conservatively by
monitor- ing H&H and bed rest for five
days, major injuries or hemodynamically
unstable require surgical repair, flu- ids also
given. Liver injury can cause hemorrhage.
Only will do surgery if injury was severe.
Injuries to the Spleen Left upper quadrant pain,
peritoneal ir- ritation, referred
left shoulder pain (Kehr’s
Same as liver injuries. In addition patients
may re- quire immunizations. Every effort is
made to save the spleen. Only will do
sign) but problem in the
spleen.
Will complain of abdominal
pain.
surgery if injury was severe.
Renal trauma Costavertebral tenderness,
microscopic or gross hematuria,
bruising and ecchy- mosis
Associated with blunt trauma.
For minor injuries bed rest, hydration and
monitoring of renal function
Major injuries may require surgical
interventions such as surgeries to control
bleeding, repair the injury or nephrectomy
o 95% decisions are made by surrogates not actually themselves that is why it is important to
have Will’s and Power or Attorney, You need to know what the patient wants and who will
appoint care.
Dimension Definition
Palliative Care Interventions to relieve symptoms of illness or injury that will
negatively affect pa- tient. Symptoms include pain, anxiety, hunger,
thirst, dyspnea, diarrhea, nausea, confusion agitation and sleep
disturbances. Often includes basic nursing interven- tions such as
repositioning, hygiene, skincare and creation of a peaceful environ-
ment. Pharmacological vs non-pharmacological.
Communication and Conflict
Resolution
Clear, ongoing honest communication between the patient, family and
healthcare providers. This includes providing a consistent message,
allowing time for family members to express themselves and agree to
treatment plan. Be clear that the pa- tient is not going to be
abandoned, and maintain continuity of care
Withholding, Limiting, or
Withdrawing Therapy
Commonly withheld therapies include dialysis, ventilators,
vasopressors, blood products, antibiotics. Despite the decision to
withdraw these therapies, it is impor- tant that the nurse ensures
comfort and relief of symptoms. Common therapies in- clude opioid
pain medication, sedation such as benzodiazepines, antiemetic medi-
cations, antidiarrheal medications, antidepressants, anticholinergics
(secretion management). Some patients may also be referred to
hospice.
Emotional and Psychological Care of
the Patient and Family
The emotional and psychological needs of the patients and their
family members need to be addressed. It is important to maintain a
nonjudgmental demeanor with patient/family interactions. Offer
spiritual counseling with pastoral care. Most im- portantly it is
important to maintain communication.
Caregiver Organizational Support Providing end-of-life care can be time consuming, so it is important
that staffing reflects that capability. Although, the patient may not be
receiving life sustaining therapy, the emotional, psychological and
symptomatic needs of the patient require time and attention.
Hemodynamics
· Used to assess:
o Patients tissue profusion
· Cardiac output
o Stroke Volume x HR
o Normal output 4-8L/min
o How much blood is ejected from the heart in one minute.
· Cardiac Index
· HR
o Too quick (tachy) ventricles do not have enough time to fill
▪ Need to slow down the heart (cardioversion, cadizem, adenosine)
o Too slow (brady) not enough blood is being pumped to the body
▪ Speed the heart up (pacemaker, epi, dopamine, atropine)
Components of Cardiac Output
· Increases in heart rate affect cardiac output. If heart is too slow affects heart rate output.
· Cardiac output will be affected by 4 specific things:
· Preload (Volume)
o Amount of blood in your ventricles at the end of diastole. Blood in your heart before it contracts
o Frank-starling:
▪ Greater the volume, the greater the stretch on the hear/ventricles (normal
physiological stretch), the greater/stronger the contraction
▪ The amount of volume, which the heart can handle, is only good.
▪ Overly stretched is not good! (CHF, cardiomegaly, HTN). We get more volume in heart,
but the heart beats less effective.
o Increased Preload
▪ Increased volume
▪ Cause:
· Fluid overload, CHF, problems with heart valves
▪ Clinical manifestations:
▪ Right side of the heart you will have cm’s in the body, if you have left side of the heart
you have cm’s in the left side of the heart.
· Right side (Increased CVP) – CVP looks at pressure
o Generalized/peripheral edema
o JVD, Ascites
· Left side (Increased PAOP/PAWP) – pulmonary artery occlusive pressure and
pulmonary artery wedge pressure
o Crackles, SOB, pulmonary edema,
o Pink frothy sputum, tachpnic
▪ Treatment
· Diuretics
o Decreased Preload (decreased CVP)
▪ Caused
· Vasodilation
· Shock
▪ Clinical Manifestation
· Flushed, warm, low BP, sweaty, diaphoretic, bounding
▪ Treatment
· Vasoconstriction – to help return blood back to the heart better
· Fluids
· Contractility
o Affects cardiac output as well
o The force of the contractions of your heart. How well is your heart pumping.
o Increased Contractility
▪ Causes
· Stimulants, stress, medications, pain, anxiety
▪ Clinical Manifestation
· Bounding pulses, HTN
▪ Treatment
· We usually do not treat. Only if someone is extremely hypertensive
· Treat the cause
o Decreased Contractility
▪ Heart not contracting effectively
▪ Causes
· MI
· Conduction system problems
· Infarction, ischemia, hypoxia, HF
· Increase in Electrolyte imbalances Potassium (Hyperkalemia)
▪ Clinical Manifestations
· Decreased tissue profusion
· Weak thready pulses, LOC changes, low BP, decreased urine output, cool
clammy skin, hypoten- sion, dyspnea,
▪ Treatment
· Positive iontropic drugs (digoxin) – increases contractility
· Blood Pressure
o Cardiac output x SVR