

Helicobacter pylori
Helicobacter pylori
Dr.B.Boyle







Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Community
Ask the community for help and clear up your study doubts
Discover the best universities in your country according to Docsity users
Free resources
Download our free guides on studying techniques, anxiety management strategies, and thesis advice from Docsity tutors
basics of h pylori for the university students and researchers
Typology: Lecture notes
1 / 35

This page cannot be seen from the preview
Don't miss anything!
Objectives: to have a clear understanding of disease caused by
Helicobacter pylori in terms of the above headings
2
2
2
Infection occurs worldwide
Prevalence will depend on the country and population
groups
Overall prevalence strongly correlates with socio-
economic conditions
In Middleaged adults in developing countries
prevalence is 80%, in industralised countries 20-50%
( rate of acquistion decreasing)
Acquisition: Oral Ingestion of the bacterium
Transmission: Within families in early childhood, not
isolated from water etc, e
H.pylori infection in
adults is usually chronic
without specific therapy:
on the other hand ,
spontaneous elimination
of the bacterium in
childhood is probably
relatively common
NEJM , Vol. 347, No. 15
Oct 10, 2002
mm.HH
Figure 2. Pathogen–Host Interactions in the Pathogenesis of
Helicobacter pylori Infection.
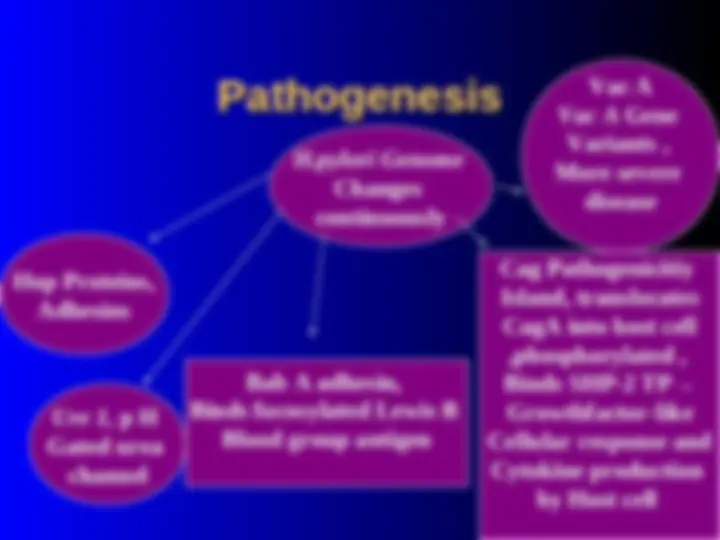
H.pylori Genome
Changes
continuously
Hop Proteins,
Adhesins
Ure 1, p H
Gated urea
channel
Vac A
Vac A Gene
Variants ,
More severe
disease
Bab A adhesin,
Binds fucosylated Lewis B
Blood group antigen
Cag Pathogenicitiy
Island, translocates
CagA into host cell
,phosphorylated ,
Binds SHP-2 TP→
Growthfactor-like
Cellular response and
Cytokine production
by Host cell
3
Figure 2. Pathogen–Host Interactions in the Pathogenesis of
Helicobacter pylori Infection.
H.pylori causes continuous gastric inflammination in
virtually all infected persons
Host response triggered by attachment to gastric
epithelium (Class II MHC-apotosis)
Initially neutrophils then T and B cells,plasma cells and
macrophages
Role of cag-PAI( Stronger response IL8) and transolation
of Cag A into gastric cells, Urease contributes
Infected gasric epithelium have increased levels of
interleukin-1ß, interleukin-2,interleukin 6, interleukin-
and TNFà.Interleukin 8 key role
(Duodenal Ulcer ,H.pylori infected )
↠ Hypersecretion Acid
Bacterial products e.g Urea
Inflammatory mediators e.g
Interleukin 1B, TNF)
Histamine relase from Mast cells
6x↑Gastrin Releasing Peptide( mediates release of Gastrin, group of
Peptide hormones produced by antral G cells), more if Cag A +
strain
May be genetic determinant of more response to Gastrin
(if D.U ↑ basal secretion of acid secretion)
Low gastric somatostain level
↑HyperGastrinaemia ↑Pariental cells mass( body)