


Geriatrics Rounds
Docsity.com















Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Community
Ask the community for help and clear up your study doubts
Discover the best universities in your country according to Docsity users
Free resources
Download our free guides on studying techniques, anxiety management strategies, and thesis advice from Docsity tutors
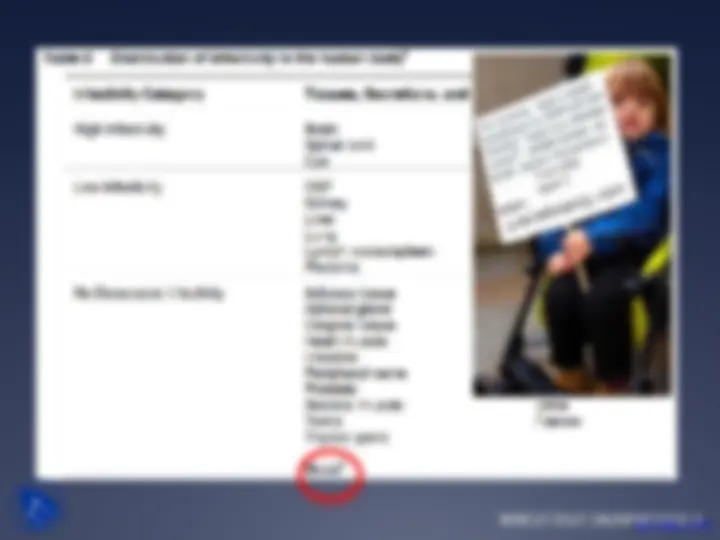
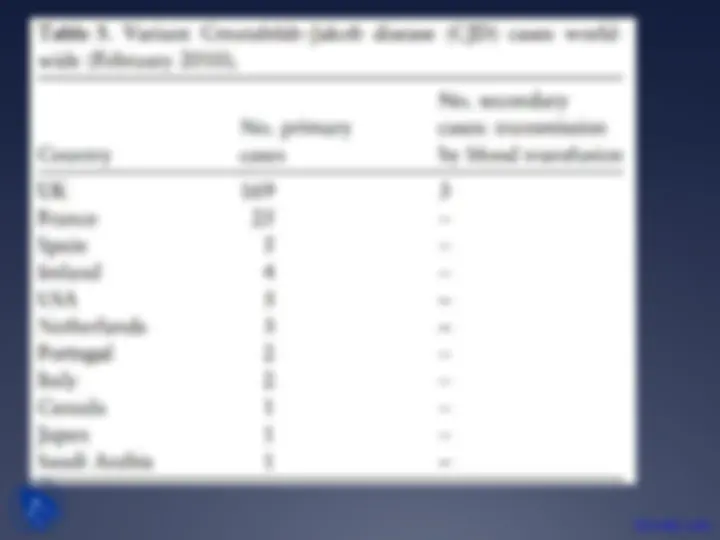
Detailed information about a 71-year-old male patient with a history of multiple health conditions who was referred to neurology for incoordination. The patient's medical history, symptoms, exam results, differential diagnoses, investigations, and eventual diagnosis of creutzfeldt-jakob disease (cjd). The document also discusses the various types of cjd, their causes, and prevalence.
Typology: Slides
1 / 44

This page cannot be seen from the preview
Don't miss anything!
22 Feb 2011: back to ER
Progressive symptoms:
Weight loss 15 lbs over 6 weeks
Chronic cough
Hematuria (occasionally)
Blood on toilet paper since ASA ( x 3 weeks)
Cerebellar Exam
Gait:
Localization?
Differential?
Investigations?
Course in Hospital:
23 Feb 2011 : MOCA 30/
24 Feb 2011:Worsening of cerebellar findings bilaterally
EEG done
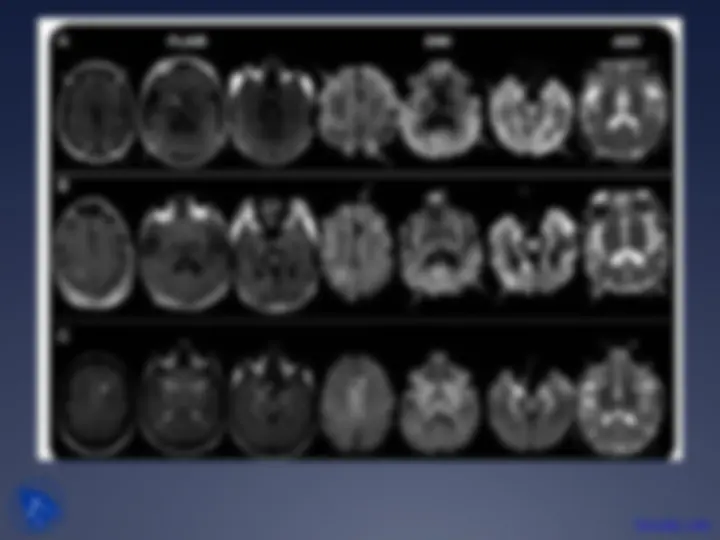
Over next week: Increasing dysphagia to solids Increased Lt hand spasticity, tremor, slurred speech Lt hand/leg myoclonic jerks, Startle reflex -ve Worsening Lt UE/LE strenght 4-/5, worsening of gait/ motility Pronounced Lt facial droop Mild behavioral changes/ paranoia: noted by family
07 March 2011 MOCA: 18/30( visuospatial/executive, attention , language)
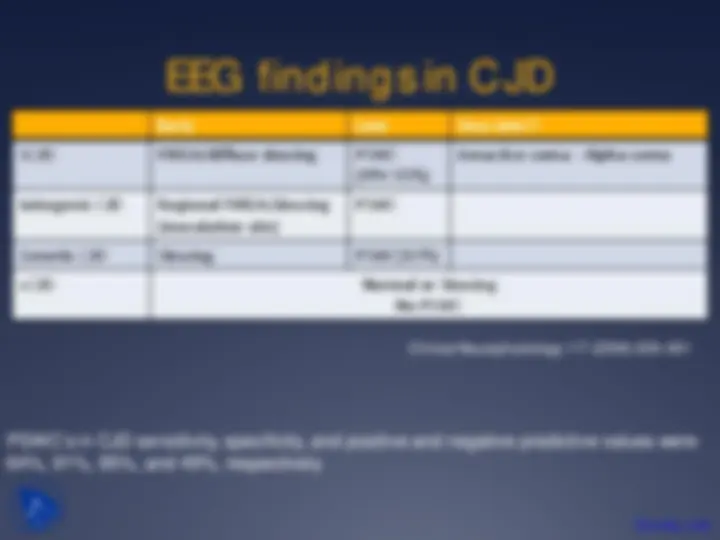
08 March 2011: EEG: Intermittent 1 Hz periodic discharges, max Rt , background slowing
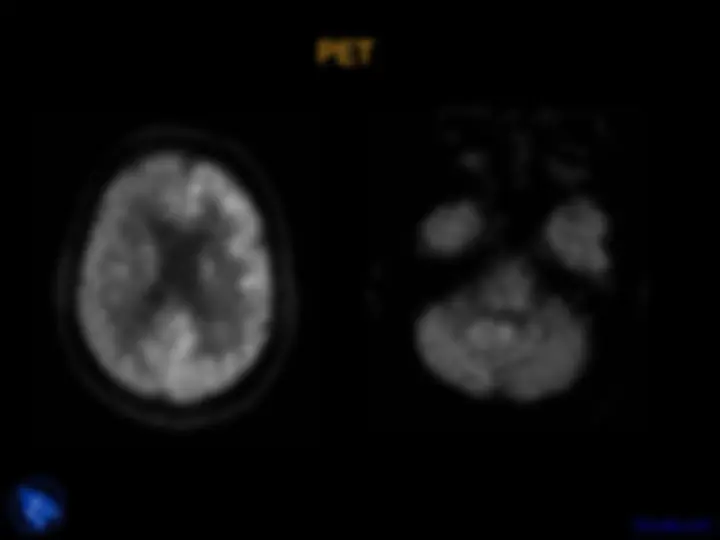
PET
PET
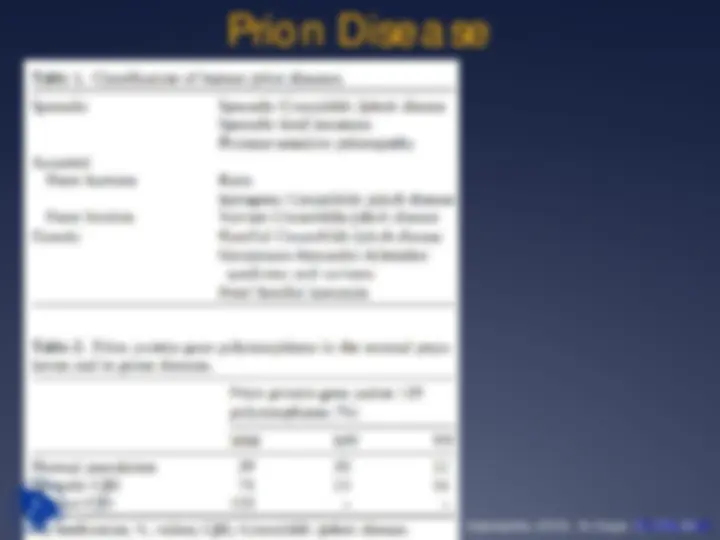
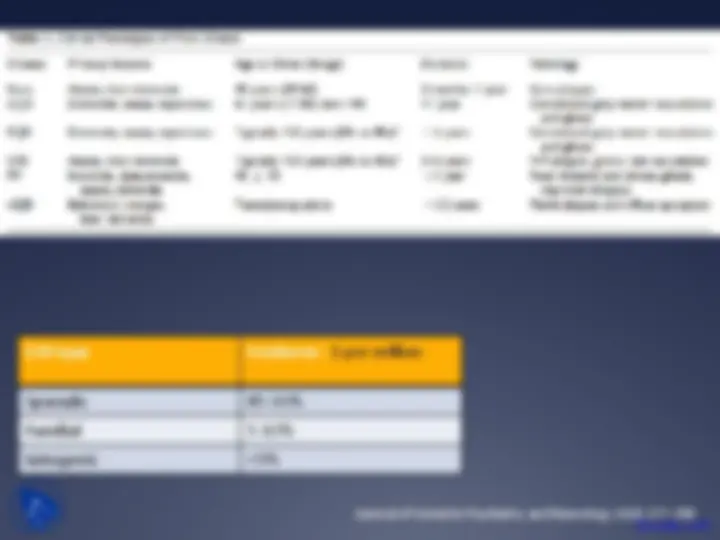
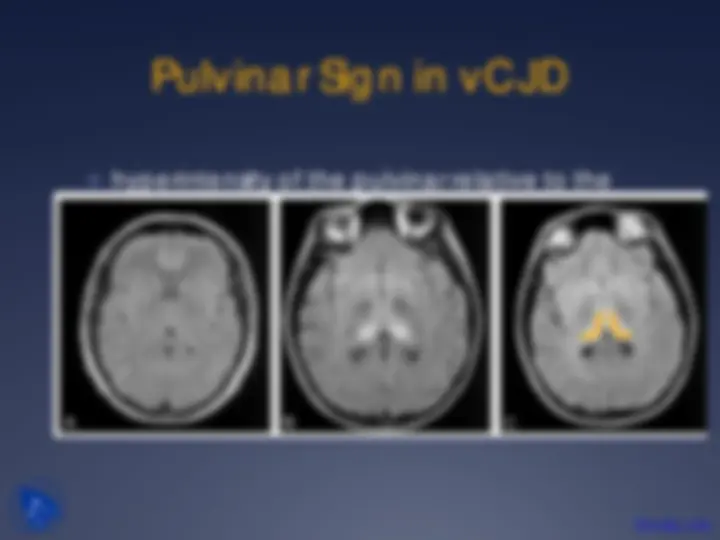
Creutzfeldt-Jakob Disease
Prion Disease
Prion: small infectious pathogen containing protein but lacking
nucleic acid
Non-pathological membrane bound protein in neuronal and non-
neuronal cells
Conversion to active, accumulating isomer
Intracellular accumulation of prions = apoptosis, cell death,
degenerative neurologic disease
CJD (and variants), kuru, Gerstmann-Straüssler-Scheinker
syndrome, familial fatal insomnia