


Dementia Diagnosis and Treatment in
Primary Care
Docsity.com











Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Community
Ask the community for help and clear up your study doubts
Discover the best universities in your country according to Docsity users
Free resources
Download our free guides on studying techniques, anxiety management strategies, and thesis advice from Docsity tutors
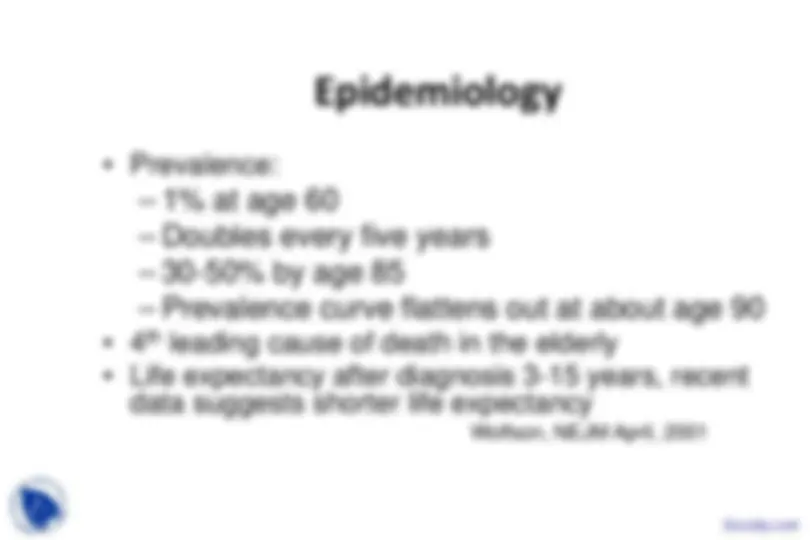
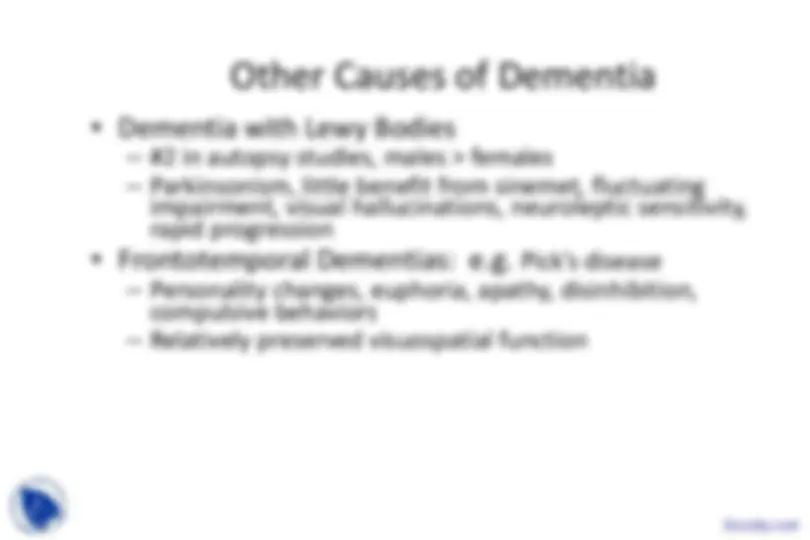
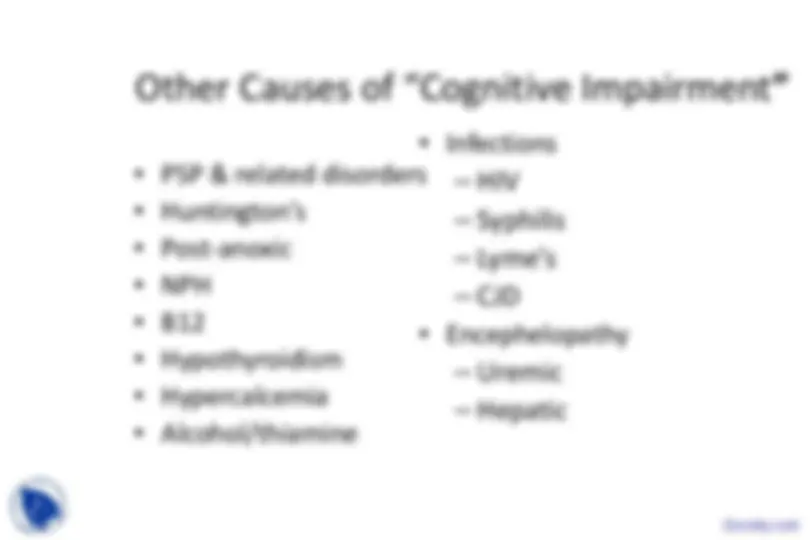
Dementia Diagnosis, Treatment in Primary Care, Epidemiology of Alzheimer, Chromosomal Defects, Head Trauma, Vascular Dementias, Hyperlipidemia, Ischemic Stroke Survivors are some important points from lecture of Introduction to Geriatrics.
Typology: Slides
1 / 38

This page cannot be seen from the preview
Don't miss anything!
Clarfield1994, Larson 1985, Patterson 1999, Freter 1998